Bronchiolitis in infants: assessment, supportive care and admission criteria
Bronchiolitis is a classic UKMLA topic—it's basically the "bread and butter" of pediatric respiratory medicine. It's most commonly caused by the Respiratory Syncytial Virus (RSV) and typically affects infants under 2 years old, peaking between 3 and 6 months.
Let me pull up some high-yield lessons that cover the NICE guidelines for assessment and management.
📚 Bronchiolitis Lessons
When you're assessing these little ones, you're usually looking for a coryzal prodrome (runny nose, sneezing) that progresses to a persistent cough and increased work of breathing. On examination, the "classic" findings are fine inspiratory crackles and/or a high-pitched wheeze.
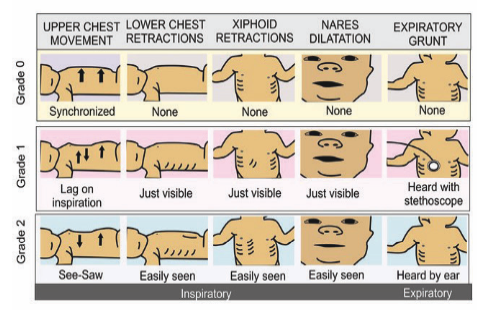
I'll find a diagram showing the signs of respiratory distress in infants, as recognizing these is key for your clinical assessment.
Recognizing the severity of respiratory distress is vital. Look for subcostal and intercostal recessions, nasal flaring, and the most concerning sign: expiratory grunting.
Now, let's talk about when to admit. This is a high-yield area for the UKMLA AKT. NICE (NG1) is very specific about the "red flags" that require hospital care.
I've summarized the admission criteria for you in this table.
| Category | Admission Criteria (NICE Guidelines) |
|---|---|
| Apnoea | Any observed or reported episodes of apnoea. |
| Oxygenation | Persistent oxygen saturations < 92% on air. |
| Feeding | Inadequate oral fluid intake (50–75% of usual volume). |
| Respiratory Effort | Severe respiratory distress (e.g., grunting, marked recessions). |
| Clinical Concern | If the clinician is concerned about the child's ability to cope at home or social factors. |
When it comes to management, the golden rule for bronchiolitis is "less is more." It’s a viral illness, so we focus entirely on supportive care.
Supportive Care Principles
- Oxygen Therapy: Indicated if saturations are persistently
< 92%. High-flow nasal cannula (HFNC) or CPAP may be used if they aren't responding to standard oxygen. - Fluid Management: If the infant is struggling to feed (remember that
< 50-75%rule), we use Nasogastric (NG) feeds or IV fluids if they can't tolerate NG. - Nasal Suctioning: Only if the nose is so congested it's interfering with feeding or causing respiratory distress.
- Safety Netting: If you're discharging them, ensure parents know to return if the child has apnoea, looks pale/blue, or is working much harder to breathe.
AKT High-Yield Tip: What NOT to do Do NOT use:
- Salbutamol or Ipratropium (they don't work for bronchiolitis)
- Corticosteroids (oral or inhaled)
- Antibiotics (unless you suspect secondary bacterial infection)
- Chest physiotherapy
Does that help clear up the assessment and management for you? If you want to test your knowledge on these criteria, I can set up a quick quiz!
Setting up chat...