Breast surgery: benign vs malignant lesions, triple assessment and management
Breast surgery is such a massive topic for the exams, but honestly, once you get the "Triple Assessment" logic down, everything else starts to click into place. It's the gold standard for evaluating any breast lump!
Let's start with how we actually approach these patients. The Triple Assessment is the backbone of diagnosis, and it's essential because no single test is 100% accurate on its own.
The Triple Assessment
- Clinical Examination: A thorough history and physical exam (palpation of the breast and axilla).
- Imaging:
- Ultrasound (USG): Preferred for women
< 35 years(denser breast tissue). - Mammography: Preferred for women
> 35 years.
- Ultrasound (USG): Preferred for women
- Pathology (Tissue Diagnosis):
- Fine Needle Aspiration Cytology (FNAC): Good for cytology, but can't distinguish between in-situ and invasive cancer.
- Core Needle Biopsy (CNB): The gold standard because it maintains tissue architecture and allows for IHC (ER/PR/HER2) markers.
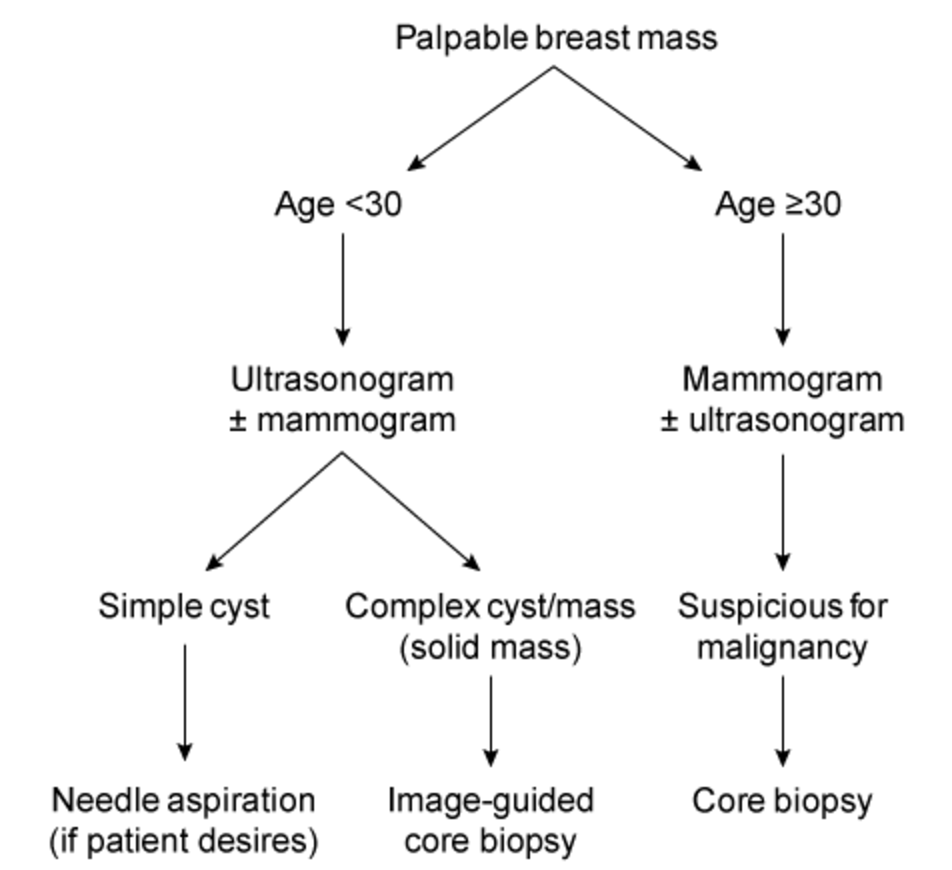
I'll pull up a quick flowchart to help you visualize this diagnostic pathway.
This flowchart perfectly summarizes how we decide between USG and Mammography based on age and what the next steps are based on those findings.
When you're examining a patient, there are some classic "red flags" that point toward malignancy. Benign lesions like Fibroadenomas (the "breast mouse") are usually mobile and smooth, whereas malignant ones are often fixed and hard.
Here's a quick comparison to help you differentiate them clinically:
| Feature | Benign (e.g., Fibroadenoma) | Malignant (Carcinoma) |
|---|---|---|
| Age | Usually younger (15-35 years) | Usually older (> 50 years) |
| Consistency | Firm, rubbery | Hard, stony |
| Mobility | Highly mobile ("Breast Mouse") | Fixed to skin or chest wall |
| Margins | Well-defined, smooth | Irregular, poorly defined |
| Skin Changes | Usually none | Peau d'orange, tethering, ulceration |
| Nipple | Normal | Retraction, bloody discharge |
| Lymph Nodes | Usually not palpable | Often palpable (Axillary) |
Management Principles
Management depends heavily on the diagnosis:
-
Benign Lesions:
- Fibroadenoma: If small and asymptomatic, we can just observe. If it's large (> 3 cm) or the patient is anxious, we can do an Excision Biopsy.
- Breast Cysts: Simple cysts can be aspirated if symptomatic. If the fluid is bloody or the cyst recurs, it needs further investigation.
- Phyllodes Tumor: These are tricky! Even "benign" ones need a wide local excision (1 cm margin) because they have a high recurrence rate.
-
Malignant Lesions (Breast Cancer):
- Breast Conserving Surgery (BCS): Lumpectomy + Axillary clearance + Radiotherapy (mandatory with BCS).
- Modified Radical Mastectomy (MRM): Removal of the breast and axillary lymph nodes (levels I and II), but preserving the Pectoralis major muscle.
- Systemic Therapy: Depending on the markers (ER/PR/HER2), we use chemotherapy, hormonal therapy (like Tamoxifen or Anastrozole), or targeted therapy (Trastuzumab).
I've got some great lessons and flashcards that cover these in much more detail. Let me pull those up for you!
📚 Breast Surgery Lessons
Those lessons cover everything from the initial workup to the complex surgical decisions for cancer. To really lock this in, let's look at some flashcards that focus on the high-yield facts you'll need for the exam.
🗂️ Breast Surgery Flashcards
Tap to study 1 flashcard in the Oncourse app
That should give you a solid foundation for breast surgery! The key is to always remember the Triple Assessment—it's the most common way these questions are framed.
If you're feeling confident, we could try a quick Clinical Rounds case to see how you'd manage a patient in the clinic, or I can pull up some PYQs (Previous Year Questions) to see how this topic has been tested recently. What do you think?
Setting up chat...