Breast lumps: triple assessment, BIRADS and management pathway
Breast lumps are a massive topic for the UKMLA AKT, and honestly, they're one of those areas where having a solid "mental algorithm" makes life so much easier. Let's start by pulling up some key lessons to give us a good foundation.
📚 Breast Lump Lessons
The Triple Assessment is the gold standard for evaluating any suspicious breast lump. The goal is to achieve 100% diagnostic accuracy by combining three different modalities. If any one of these is suspicious, you proceed as if it's malignant until proven otherwise.
- Clinical Assessment: A thorough history (risk factors, cycle relation) and bilateral breast examination (including axillary lymph nodes).
- Imaging:
- Age < 35: Ultrasound is preferred because younger breast tissue is often too dense for mammography.
- Age ≥ 35: Mammography is the primary tool, often supplemented by ultrasound.
- Tissue Sampling:
- Core Biopsy: The preferred method as it preserves tissue architecture (allows differentiation between in situ and invasive cancer).
- Fine Needle Aspiration (FNA): Mostly used for cysts or sometimes for axillary nodes, but less common for the primary lump now.
Let me find a visual to help you visualize what we're looking for during the imaging phase.
That mammogram really highlights the difference between normal fibroglandular tissue and a suspicious, high-density mass.
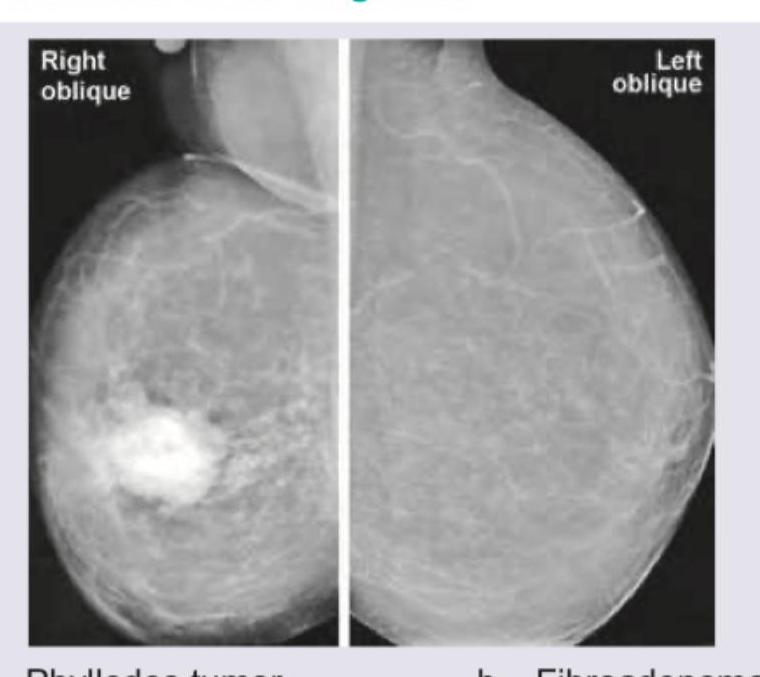
This image shows a classic "spiculated" mass on the right, which is highly suggestive of malignancy.
When radiologists look at these images, they use the BI-RADS (Breast Imaging-Reporting and Data System) to standardize their findings. It's a 0-6 scale that tells the clinician exactly how worried they should be.
| BI-RADS Score | Assessment | Management Recommendation |
|---|---|---|
| 0 | Incomplete | Needs further imaging (e.g., specialized views, US) |
| 1 | Negative | Routine screening |
| 2 | Benign | Routine screening (e.g., simple cyst, fibroadenoma) |
| 3 | Probably Benign | Short-interval follow-up (usually 6 months) |
| 4 | Suspicious | Biopsy should be considered |
| 5 | Highly Suggestive of Malignancy | Appropriate action (Biopsy/Surgery) is required |
| 6 | Known Biopsy-Proven Malignancy | Surgical excision when clinically appropriate |
In the UK, the management pathway is heavily driven by the NICE 2-week wait (2WW) referral criteria. If a patient meets these criteria, they must be seen by a specialist within 14 days for that triple assessment we talked about.
NICE 2WW Referral Criteria (High Yield!):
- Age ≥ 30 with an unexplained breast lump (with or without pain).
- Age ≥ 50 with unilateral nipple symptoms (discharge, retraction, etc.).
- Skin changes (e.g., peau d'orange) or a suspicious axillary lump.
Once they're in the clinic, the pathway usually follows a very logical flow from assessment to diagnosis. Let me map that out for you with a flowchart.
That flowchart really sums up the whole process! The key is that Triple Assessment is the core of the diagnostic workup, and the BI-RADS score helps guide the next steps.
One thing to keep in mind for the UKMLA is the difference between a fibroadenoma (common in younger women, "breast mouse," mobile, firm) and a breast cyst (common in peri-menopausal women, often fluctuates with the menstrual cycle).
Since we've covered a lot of ground, would you like to try a quick game to see if you can categorize different breast lump features? It's a great way to lock in the differences between benign and malignant findings!
Setting up chat...