Bipolar disorder: mania vs hypomania, lithium monitoring and mood stabilisers
Hey! Bipolar disorder is an absolute staple for the UKMLA AKT. The examiners love to trip people up on the nuances between mania and hypomania, and the lithium monitoring rules are basically guaranteed marks if you know them.
Let's start with a quick breakdown of the "highs" so you can spot them easily in a clinical vignette.
| Feature | Hypomania | Mania |
|---|---|---|
| Duration | At least 4 days | At least 7 days |
| Social/Work Impact | Mild; does not require hospitalisation | Severe; usually requires hospitalisation |
| Psychotic Symptoms | Never present | May be present (e.g., delusions of grandeur) |
| Functional Impairment | Not severe enough to cause total social/occupational breakdown | Significant impairment; often leads to risky behaviour |
Lithium is the "gold standard" mood stabiliser, but it's a high-risk drug with a narrow therapeutic index. For the AKT, you need to know these monitoring rules like the back of your hand:
- Levels: Check 12 hours post-dose.
- Range: Aim for 0.4–1.0 mmol/L.
- Toxicity: Usually occurs above 1.5 mmol/L.
- Frequency: Weekly until stable, then every 3 months.
- Other tests: Check TFTs, U&Es, and Calcium every 6 months (Lithium can cause hypothyroidism, renal failure, and hyperparathyroidism).
Let me pull up some detailed lessons on Bipolar management and Lithium for you.
📚 Bipolar Management Lessons
Those lessons are great for the deep dive, but here are the "must-know" side effects for the other mood stabilisers:
- Valproate: ==Highly teratogenic==. In the UK, it must never be used in women of childbearing potential unless a Pregnancy Prevention Programme (PPP) is in place.
- Lamotrigine: Watch out for a rash! It can cause Stevens-Johnson Syndrome (SJS), so it's started at a very low dose and titrated slowly.
- Carbamazepine: A potent P450 enzyme inducer (interacts with everything!) and can cause agranulocytosis.
Visuals always help me remember the side effects better. Let me find a good diagram for you.
Here's a visual guide to those Lithium and Valproate toxicities. Remember: ==Lithium toxicity is often precipitated by dehydration, NSAIDs, or ACE inhibitors== (anything that messes with renal clearance).
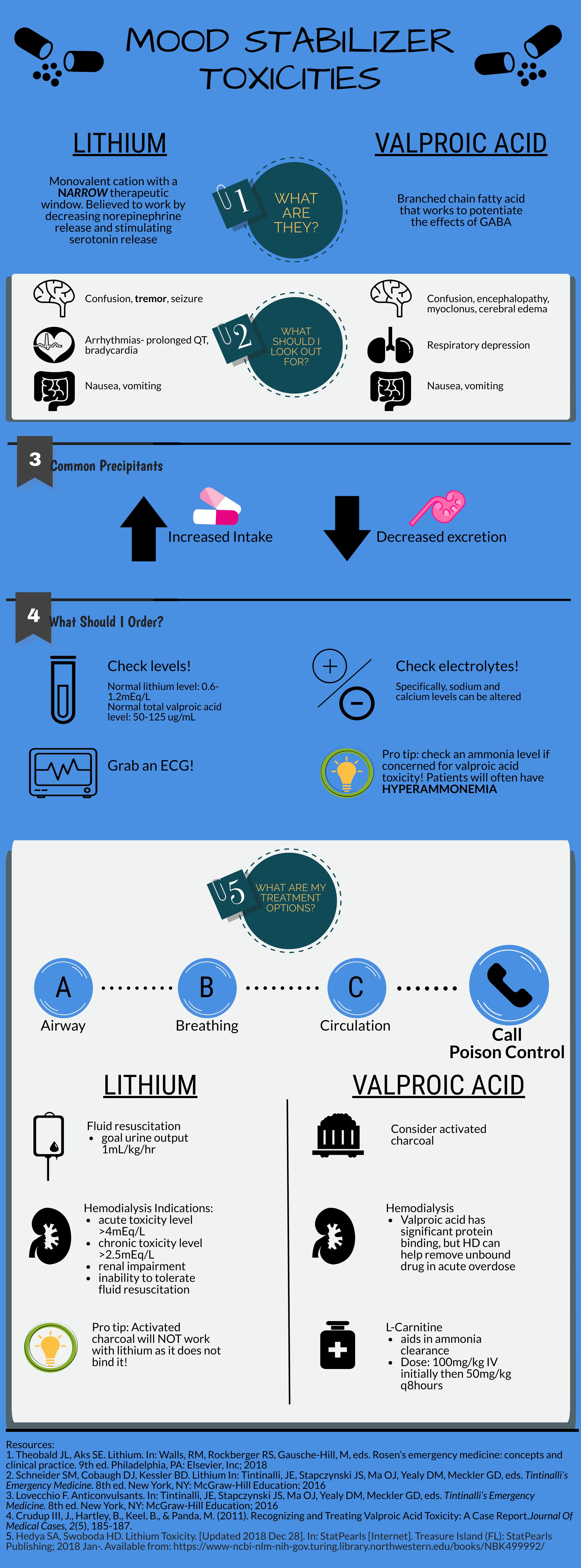
That infographic is a lifesaver for those "what's the next step?" questions. Just to wrap up, here are the classic signs of Lithium Toxicity to watch for in a clinical vignette:
- Early signs: Coarse tremor (different from the fine tremor seen at therapeutic levels), nausea, and vomiting.
- Late signs: Ataxia, confusion, seizures, and even coma.
If you suspect toxicity, the first step is to stop the Lithium and check the serum levels, U&Es, and ECG. Severe cases might even need haemodialysis!
Hope that helps you smash those psychiatry questions! Let me know if you want to dive deeper into any of these.
Setting up chat...