Bariatric surgery: indications, procedures and metabolic outcomes
Bariatric surgery has really evolved from being just "weight loss surgery" to "metabolic surgery" because of how effectively it handles conditions like Type 2 Diabetes. It's a heavy-hitter in the management of morbid obesity.
Let's break this down into the clinical indications, the common procedures we see in the wards, and those all-important metabolic shifts.
1. Indications (Who qualifies?)
The criteria are strictly based on Body Mass Index (BMI) and associated comorbidities. According to the standard guidelines (often tested in NEET-PG/INI-CET):
- BMI ≥ 40 kg/m²: Even without any other health issues.
- BMI ≥ 35 kg/m²: If they have at least one major obesity-related comorbidity (e.g., Type 2 Diabetes, severe Hypertension, Obstructive Sleep Apnea, or NAFLD).
- BMI ≥ 30 kg/m²: Specifically for patients with poorly controlled Type 2 Diabetes (this is the "metabolic surgery" threshold).
2. Common Surgical Procedures
We generally categorize these into restrictive, malabsorptive, or a mix of both.
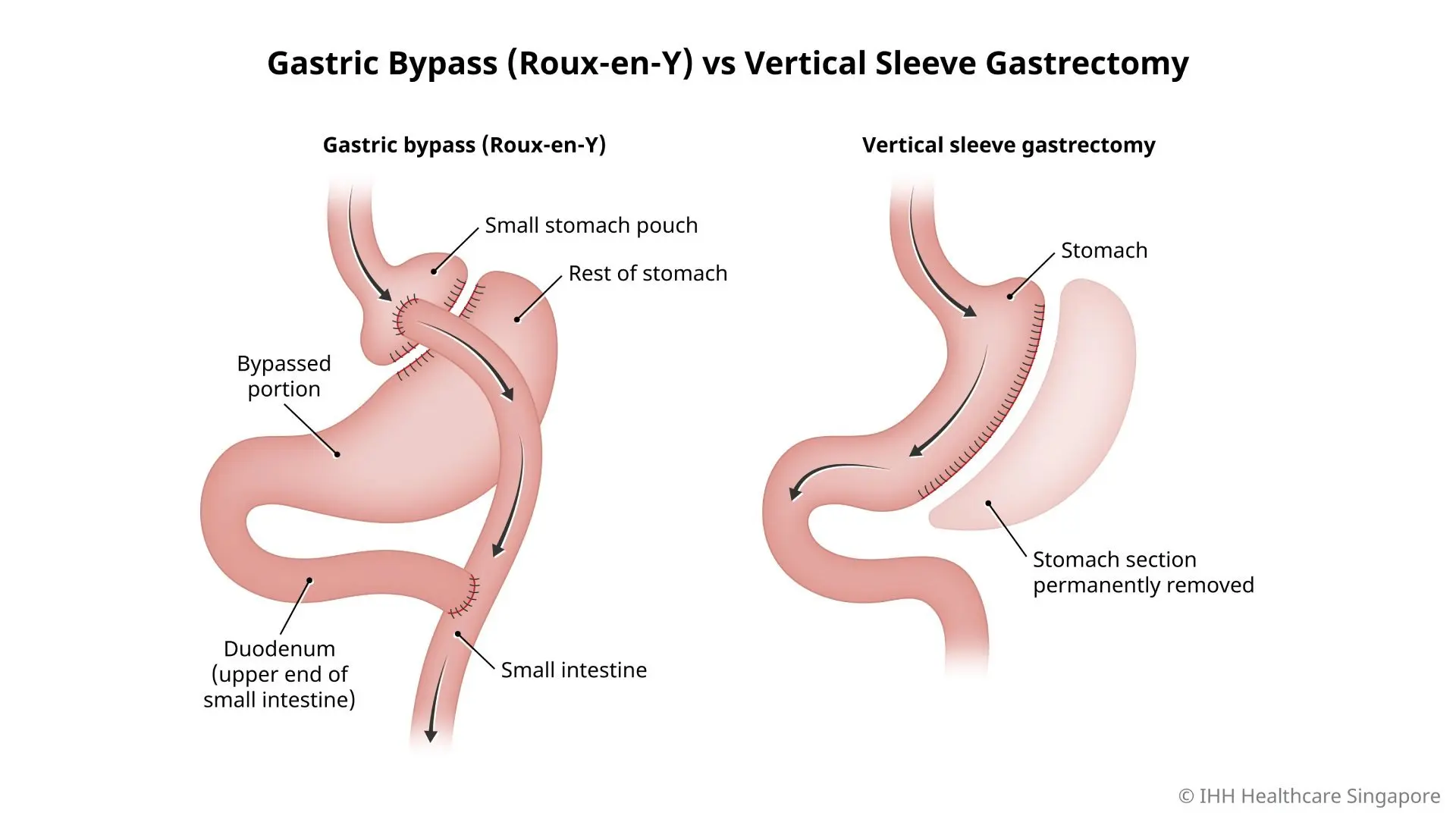
- Sleeve Gastrectomy (Restrictive): The most common procedure today. About 80% of the stomach is removed, leaving a "sleeve" or tube. It also reduces Ghrelin (the hunger hormone) because the fundus is removed.
- Roux-en-Y Gastric Bypass (RYGB) (Combined): The "Gold Standard." A small stomach pouch is created and connected directly to the jejunum. This bypasses the rest of the stomach and the duodenum.
- Adjustable Gastric Banding (Restrictive): Less common now due to long-term complications, but involves placing a band around the upper stomach.
- Biliopancreatic Diversion with Duodenal Switch (BPD/DS): Mostly malabsorptive; reserved for very high BMI cases.
3. Metabolic Outcomes
This is where the magic happens. It’s not just about eating less; it’s about hormonal rewiring.
- Diabetes Remission: Often happens before significant weight loss occurs, especially with RYGB. This is due to increased GLP-1 and PYY levels.
- Lipid Profile: Significant reduction in triglycerides and LDL, with an increase in HDL.
- Hypertension: Often improves or resolves completely within months.
- Hormonal Shift: Decrease in Insulin resistance and Leptin; decrease in Ghrelin (especially in Sleeve).
I'll pull up some high-yield lessons on these procedures so you can see the anatomical differences and the specific complications (like Dumping Syndrome) that often show up in exams.
📚 Bariatric Surgery Lessons
To help you visualize the anatomical changes, I'll find a diagram comparing the Sleeve Gastrectomy and the Roux-en-Y Gastric Bypass. Seeing the "bypass" part of the RYGB really helps in understanding why it causes more malabsorption and nutritional deficiencies (like B12 and Iron) compared to the Sleeve.
I've found a great diagram that compares the two most common procedures. Notice how the Roux-en-Y creates a tiny pouch and a "Y" junction, which is why it's so effective for weight loss but also why patients need lifelong vitamin supplementation.
One thing that often comes up in exams is the Dumping Syndrome (especially after RYGB). It happens because the pylorus is bypassed, and high-osmolarity food (like sugar) hits the small intestine too fast.
- Early Dumping (15-30 mins): Due to fluid shift into the gut (tachycardia, palpitations, abdominal pain).
- Late Dumping (1-3 hours): Due to a massive insulin surge causing reactive hypoglycemia.
Since this is a high-yield topic for surgery and medicine, would you like to try a few practice questions to see how these concepts are tested?
Setting up chat...