Atrial fibrillation: CHA2DS2-VASc score, rate vs rhythm control
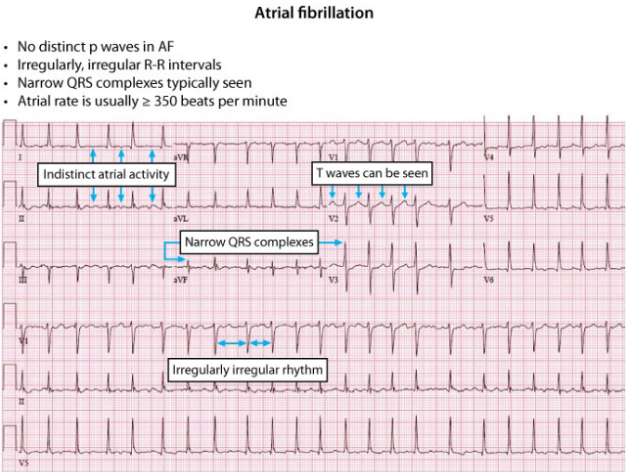
Ah, Atrial Fibrillation (AF)—the classic "irregularly irregular" rhythm that's a staple for the UKMLA AKT. It's all about managing the risk of stroke while keeping the heart rate (or rhythm) under control. Let's start by looking at what AF actually looks like on an ECG so we're on the same page.
That ECG perfectly shows the "irregularly irregular" rhythm and the lack of distinct P waves. Now, the first thing we worry about in AF is the risk of a thromboembolic stroke. To decide if a patient needs anticoagulation (usually a DOAC like Apixaban), we use the CHA2DS2-VASc score.
The CHA2DS2-VASc score is our go-to tool for assessing stroke risk. For the AKT, remember: Offer anticoagulation if the score is 2 or more (consider it if the score is 1 in men).
Here's the breakdown of the scoring:
| Letter | Risk Factor | Points |
|---|---|---|
| C | Congestive Heart Failure (or LV dysfunction) | 1 |
| H | Hypertension | 1 |
| A2 | Age ≥ 75 years | 2 |
| D | Diabetes Mellitus | 1 |
| S2 | Stroke / TIA / Thromboembolism history | 2 |
| V | Vascular Disease (Prior MI, PAD, or aortic plaque) | 1 |
| A | Age 65–74 years | 1 |
| Sc | Sex Category (Female) | 1 |
Once you've sorted the stroke risk, the next big question is: Rate or Rhythm control?
In most cases (especially older patients or those with minimal symptoms), rate control is the first-line choice. We usually aim for a resting heart rate of < 90 bpm (or < 110 bpm if they're asymptomatic).
Here's how to decide between the two:
| Strategy | When to Choose | First-Line Drugs |
|---|---|---|
| Rate Control | First-line for most (>65, asymptomatic, or sedentary) | Beta-blockers (e.g., Bisoprolol) or Calcium channel blockers (e.g., Diltiazem/Verapamil) |
| Rhythm Control | Younger patients (<65), symptomatic despite rate control, or AF with a reversible cause | Beta-blockers (first-line), Flecainide (if no structural heart disease), or Amiodarone |
This is a high-yield topic for the AKT, so it's worth diving into the details. I'll pull up some relevant lessons and flashcards to help you lock this in.
📚 AF Management Lessons
Those lessons cover everything from the basics to the more complex management. To really test your recall, let's get some flashcards on the CHA2DS2-VASc score and the rate/rhythm control drugs.
🗂️ AF Flashcards Search
Tap to study 14 flashcards in the Oncourse app
That's a lot of info, but here are the top 3 things to keep in your back pocket for the AKT:
- Anticoagulation: Always calculate the CHA2DS2-VASc score. If it's ≥ 2, offer a DOAC. If it's 1 in a male, consider it. If it's 0 (or 1 in a female with no other risk factors), you can usually skip it.
- Rate Control: This is the default for most patients. Beta-blockers or CCBs are your first-line choices.
- Rhythm Control: Think about this for younger patients, those with a clear trigger (like an infection), or if rate control isn't cutting it.
If you want to practice applying this to a clinical scenario, I can set up a quick Clinical Rounds case for you! Just let me know.
Setting up chat...