Asthma: BTS/SIGN stepwise management, peak flow and action plans
Asthma management is a bread-and-butter topic for the UKMLA AKT, and the BTS/SIGN guidelines are the gold standard you'll need to know inside out. It's all about that stepwise approach—escalating care when symptoms aren't controlled and stepping down when things have been stable for a while.
Let's break down the management steps, how we use Peak Expiratory Flow (PEF), and what goes into those all-important action plans.
1. BTS/SIGN Stepwise Management (Adults)
The goal is "no daytime symptoms, no night-time awakening, and no need for rescue medication." If a patient is using their SABA (blue inhaler) three times a week or more, it’s time to move up a step.
- Step 1: Mild intermittent asthma
- Inhaled short-acting $\beta_2$ agonist (SABA) as required (e.g., Salbutamol).
- Step 2: Regular preventer therapy
- Add inhaled corticosteroid (ICS) at a low dose (e.g., Beclometasone 200-400 $\mu$g/day).
- Step 3: Initial add-on therapy
- Add an inhaled long-acting $\beta_2$ agonist (LABA) (e.g., Salmeterol).
- Note: If the LABA helps but control is still inadequate, increase the ICS dose. If the LABA doesn't help at all, stop it and increase the ICS dose.
- Step 4: Persistent poor control
- Increase ICS to medium dose OR add a Leukotriene Receptor Antagonist (LTRA) like Montelukast, or a LAMA (Tiotropium), or Theophylline.
- Step 5: Continuous or frequent use of oral steroids
- Maintain high-dose ICS and use daily oral corticosteroids (Prednisolone). Refer to specialist care.
2. Peak Flow Monitoring
Peak flow is our objective measure of airway obstruction. For the AKT, remember these key points:
- Diurnal Variation: A variation in PEF of >20% is highly suggestive of asthma.
- Personal Best: Management is ideally based on the patient's "personal best" peak flow rather than just predicted values.
- Acute Severity: In an acute attack, PEF is used to grade severity (e.g., Moderate is >50-75% best/predicted, Acute Severe is 33-50%, and Life-threatening is <33%).
3. Personalised Asthma Action Plans (PAAP)
Every patient should have a written PAAP. It’s a game-changer for reducing hospital admissions. It usually follows a "traffic light" system:
- Green (Routine): When feeling well. Explains daily preventer dose and SABA use.
- Amber (Getting worse): When symptoms increase or PEF drops (e.g., below 80% of best). Instructions on increasing ICS or starting a rescue course of oral steroids.
- Red (Emergency): When symptoms are severe or PEF is very low (e.g., below 50%). Instructions on when to call 999 or attend A&E.
I've got a great summary table that compares these steps and a flowchart for the diagnostic pathway if you'd like to see those next! I can also pull up some practice questions to see how this looks in an exam format.
To help you visualize the escalation of treatment, let me grab a summary table for you.
That table gives a good overview of how we classify severity to decide where to start on the "ladder."
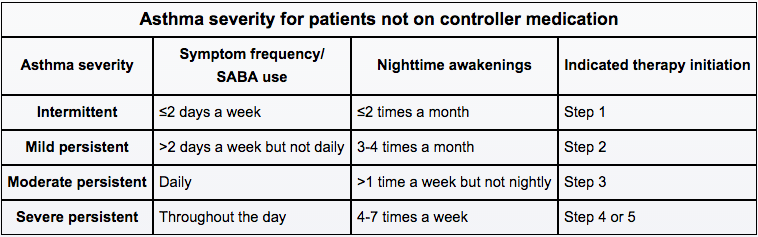
This table helps categorize asthma severity based on symptom frequency and nighttime awakenings, which directly informs which BTS/SIGN step a patient should start on.
Since you're prepping for the UKMLA, would you like to try a few practice questions on this? It's a very common topic for "next best step in management" style questions. I can also pull up some flashcards if you want to drill the specific drug doses!
Setting up chat...