Antifungal drugs: mechanisms, spectrum and clinical use comparison
Antifungals are a high-yield topic for the USMLE, especially when you start looking at systemic infections in immunocompromised patients. It's easiest to group them by where they hit the fungal cell—usually the cell membrane or the cell wall.
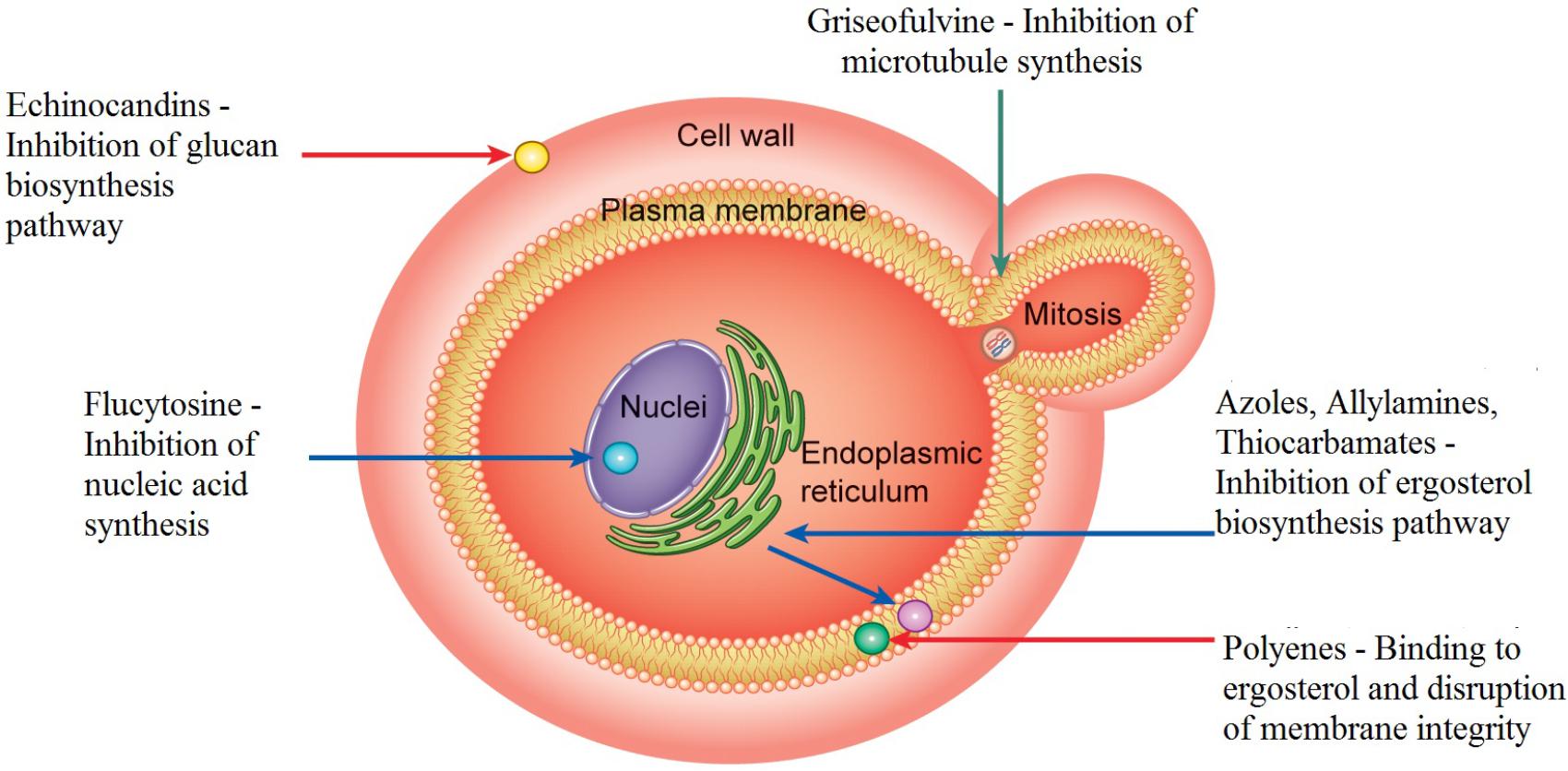
Let me find a good diagram that shows these mechanisms of action so you can visualize exactly where each drug class is working.
That diagram gives a great overview of the "battlefield." To make this easier to study, I've broken down the major classes by their mechanism, what they cover, and when we actually use them in the clinic.
| Drug Class | Mechanism of Action | Spectrum of Activity | Clinical Use / Key Notes |
|---|---|---|---|
| Polyenes (Amphotericin B, Nystatin) | Binds ergosterol; forms pores in the cell membrane | Broadest spectrum (Candida, Aspergillus, Cryptococcus, Mucor) | Amphotericin B: "Ampho-terrible" due to nephrotoxicity. Nystatin: Topical/oral swish for thrush. |
| Azoles (Fluconazole, Itraconazole, Voriconazole) | Inhibits 14-$\alpha$-demethylase (prevents ergosterol synthesis) | Broad (Candida, Cryptococcus, Dimorphic fungi) | Fluconazole: Chronic suppression of Cryptococcal meningitis. Voriconazole: 1st line for Aspergillus. |
| Echinocandins (Caspofungin, Micafungin) | Inhibits $\beta$-glucan synthesis (cell wall disruption) | Candida (including resistant strains), Aspergillus | Used for severe systemic candidemia. Generally well-tolerated. |
| Antimetabolites (Flucytosine) | Inhibits DNA/RNA synthesis (converted to 5-FU) | Cryptococcus, Candida | Always used in combination (usually with Ampho B) to prevent resistance. |
| Allylamines (Terbinafine) | Inhibits squalene epoxidase | Dermatophytes (Skin/Nails) | 1st line for onychomycosis (nail fungus). |
| Griseofulvin | Interferes with microtubule function (mitosis) | Dermatophytes | Older drug for tinea infections; induces CYP450. |
High-Yield Study Pearls
- Amphotericin B Toxicity: Remember the "shake and bake" (fever/chills) and the nephrotoxicity. It can cause hypokalemia and hypomagnesemia because it makes the renal tubules "leaky."
- Azole Side Effects: All azoles inhibit CYP450 to some degree. Ketoconazole is the big one for causing gynecomastia because it also inhibits desmolase (the first step in steroid synthesis).
- Voriconazole: Look out for the "trippy" side effects—visual disturbances (flashing lights or color changes) are a classic board exam clue.
- Echinocandins: These are the "penicillins of the fungal world" because they target the cell wall ($\beta$-glucan), which humans don't have. This makes them very low-toxicity.
I've pulled up some lessons and flashcards so you can dive deeper into the specifics of each drug class and test your memory.
🗂️ Antifungal Flashcards
Tap to study 27 flashcards in the Oncourse app
📚 Antifungal Lessons
Those lessons and flashcards cover everything from the basic pharmacology to the specific side effects you'll see on your exams.
If you're feeling confident, we could even try a quick practice quiz to see how well you can differentiate between these drugs in a clinical scenario! Just let me know if you're ready for that.
Setting up chat...