Anticoagulation: warfarin vs DOACs, INR management and reversal agents
Anticoagulation is a massive topic for the UKMLA AKT, especially since the shift towards DOACs as first-line therapy for many conditions like non-valvular Atrial Fibrillation (AF) and Venous Thromboembolism (VTE).
To get us started, I've put together a quick comparison of how these two classes of drugs stack up against each other.
| Feature | Warfarin (VKA) | DOACs (e.g., Apixaban, Rivaroxaban) |
|---|---|---|
| Mechanism | Vitamin K Antagonist (Factors II, VII, IX, X) | Direct Factor Xa or Thrombin (IIa) inhibition |
| Onset of Action | Slow (3-5 days); requires heparin bridging initially | Rapid (2-4 hours) |
| Monitoring | Regular INR monitoring required | No routine monitoring needed |
| Dosing | Variable (highly affected by diet/drugs) | Fixed dosing |
| Half-life | Long (~40 hours) | Short (7-15 hours) |
| Renal Clearance | Minimal | Significant (requires dose adjustment) |
| Food Interactions | Significant (Vitamin K intake) | Minimal (Rivaroxaban taken with food) |
Managing a high INR is a classic AKT scenario. The key is to distinguish between major bleeding, minor bleeding, and no bleeding.
INR Management (NICE/BNF Guidelines)
- Major Bleeding (any INR):
- Stop Warfarin.
- Give Prothrombin Complex Concentrate (PCC) (e.g., Beriplex, Octaplex) — this is faster and more effective than FFP.
- Give IV Vitamin K (5mg).
- Minor Bleeding (INR > 5.0):
- Stop Warfarin.
- Give IV Vitamin K (1–3mg).
- Restart when INR < 5.0.
- No Bleeding (INR 5.0 – 8.0):
- Withhold 1 or 2 doses of Warfarin.
- Reduce subsequent maintenance dose.
- No Bleeding (INR > 8.0):
- Stop Warfarin.
- Give Oral Vitamin K (1–5mg).
- Restart when INR < 5.0.
When things go wrong and we need to reverse the effects immediately, we use specific reversal agents. I've summarized the most important ones for you below.
| Anticoagulant | Specific Reversal Agent | Alternative / Supportive |
|---|---|---|
| Warfarin | Vitamin K (Phytomenadione) | PCC (Factors II, VII, IX, X) |
| Dabigatran | Idarucizumab (Praxbind) | Dialysis (it's not protein-bound) |
| Apixaban / Rivaroxaban | Andexanet alfa | PCC (if specific agent unavailable) |
| Heparin (UFH) | Protamine Sulfate | - |
| LMWH (Enoxaparin) | Protamine (partial reversal only) | - |
To help you visualize where these drugs act, let's take a look at the coagulation cascade. Understanding the "X" in Factor Xa inhibitors (like Apixaban) and the "IIa" for Dabigatran (Direct Thrombin Inhibitor) makes the mechanism much easier to remember.
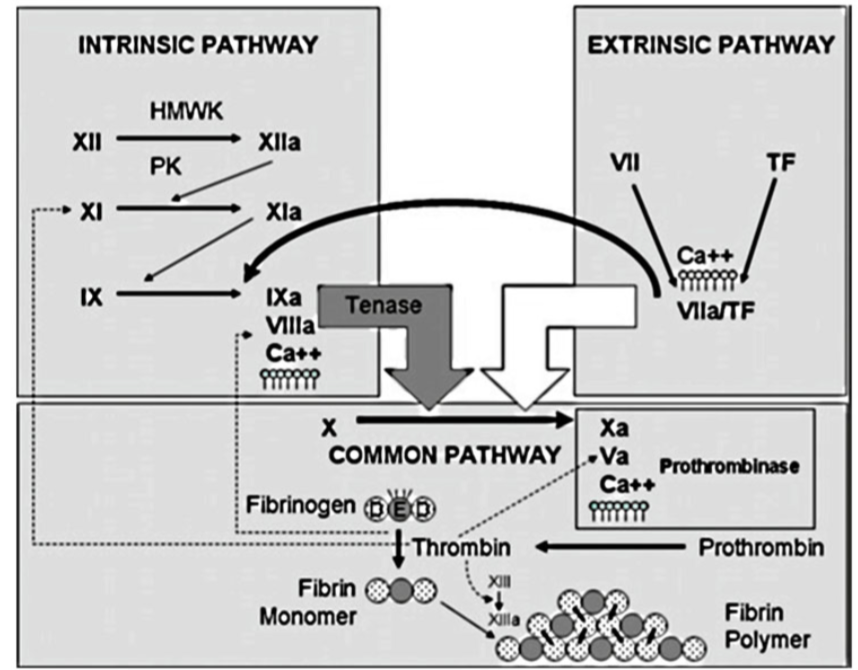
This diagram illustrates the intrinsic, extrinsic, and common pathways. Notice how Warfarin inhibits Factors II, VII, IX, and X, while DOACs target specific points like Factor Xa (Rivaroxaban, Apixaban) or Thrombin (Dabigatran).
To help you lock this in for your AKT, I've pulled some high-yield lessons and flashcards. These cover the specific indications and monitoring requirements in more detail.
🗂️ Anticoagulation Flashcards
Tap to study 9 flashcards in the Oncourse app
📚 Anticoagulation Lessons
Those lessons and flashcards should give you a solid foundation! Before we move on, here are a few high-yield "nuggets" specifically for the AKT:
- Target INR: For most conditions (AF, VTE), the target is 2.5 (range 2.0–3.0). For mechanical heart valves, it's usually higher, around 3.5 (range 3.0–4.0).
- NICE Preference: DOACs are now generally preferred over Warfarin for non-valvular AF because they have a lower risk of intracranial hemorrhage and don't require the constant "blood test dance."
- Renal Function: Always check the eGFR before starting a DOAC. If it's < 15, they are usually contraindicated, and Warfarin becomes the go-to.
Would you like to test your knowledge with a quick game, or should we jump straight into some practice questions?
Setting up chat...