Antepartum haemorrhage: placenta praevia vs abruption — comparison and management
Hey there! Antepartum haemorrhage (APH) is a massive topic for the UKMLA AKT, and being able to distinguish between placenta praevia and placental abruption is a classic exam favorite.
Let's start with a side-by-side comparison of the clinical features to help you keep them straight in a high-pressure exam scenario.
| Feature | Placenta Praevia | Placental Abruption |
|---|---|---|
| Pain | Painless bleeding | Painful bleeding (often constant) |
| Bleeding | Usually bright red, can be heavy | May be "revealed" (visible) or "concealed" (internal) |
| Uterine Tone | Soft, non-tender uterus | "Woody" hard, tense, and tender uterus |
| Fetal Heart | Usually normal (initially) | Often shows fetal distress or absent |
| Risk Factors | Previous C-section, multiparity, smoking | Hypertension, pre-eclampsia, cocaine, trauma |
| Shock | Proportionate to visible blood loss | May be out of proportion to visible loss (if concealed) |
| Engagement | Fetal head usually high/unengaged | Fetal head may be engaged |
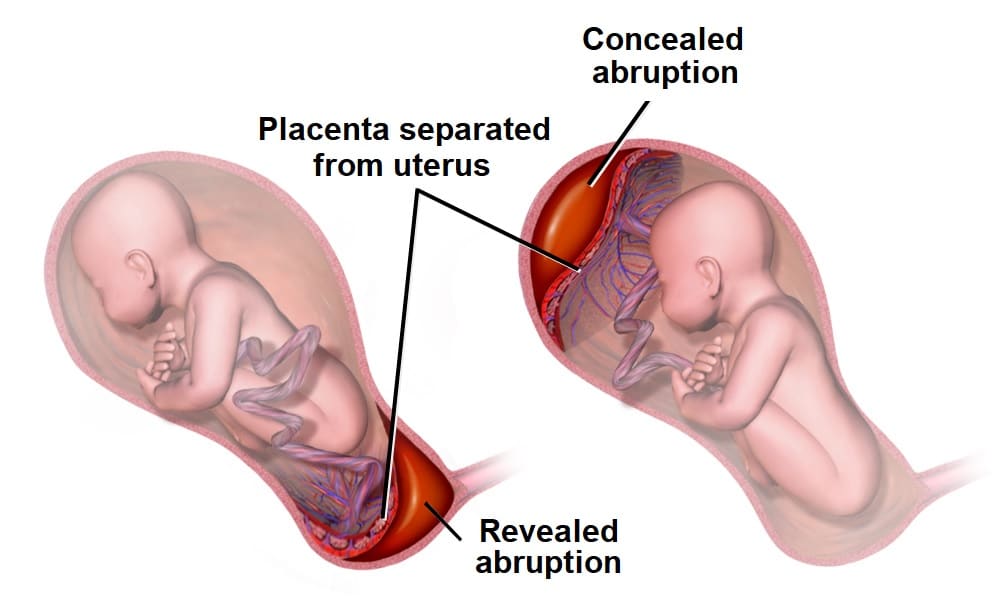
It really helps to visualize where the placenta is sitting in both scenarios. Let me find a good diagram for you to see the difference between the low-lying placenta in praevia and the separation in abruption.
That diagram is perfect for understanding how blood can be hidden in an abruption. Let me also find a quick visual for placenta praevia so you can see the different grades of low-lying placenta.
Here are the visual differences between the two. Notice how in placental abruption, the blood can be trapped (concealed), whereas in placenta praevia, the placenta is simply in the wrong place, blocking the exit.

Now, let's talk management. In the UK, we follow the RCOG Green-top Guidelines. The absolute priority is the ABCDE approach—stabilizing the mother first.
Key management points include:
- IV Access: Two large-bore cannulae (14G or 16G).
- Blood Tests: FBC, Clotting, U&Es, and Group & Save/Crossmatch (at least 4 units).
- Anti-D: If the mother is Rhesus-negative, she needs Anti-D within 72 hours of the bleed.
- Steroids: If the bleed is before 34-36 weeks, give corticosteroids (e.g., betamethasone) for fetal lung maturity.
Here's a flowchart to help you decide on the next steps based on the clinical picture.
That flowchart should help you navigate the clinical decision-making process. Remember, the key AKT differentiator is often the uterine tone (soft in praevia, woody-hard in abruption).
I've pulled up some high-yield lessons and flashcards to help you lock in these concepts for your exam.
📚 APH High-Yield Lessons
To really make sure you can recall these differences under pressure, I've also found some flashcards for you. These are great for quick-fire revision.
🗂️ APH Revision Flashcards
Tap to study 21 flashcards in the Oncourse app
I hope that helps you master APH for your AKT!
One last high-yield tip: If a patient presents with APH, never perform a digital vaginal examination until placenta praevia has been ruled out by ultrasound. Doing so could cause massive, life-threatening haemorrhage if the placenta is covering the os.
Good luck with your studies! If you want to test yourself with some practice questions or a quick game on this topic, just let me know.
Setting up chat...