Allergic rhinitis: classification, diagnosis and management
Ah, Allergic Rhinitis! The classic "sneezing and wheezing" saga. It's a bread-and-butter topic for ENT and definitely shows up in exams like NEET-PG and INI-CET. Let's break down the classification, diagnosis, and management so it sticks.
First, let me pull up some high-yield lessons that cover the essentials for your prep.
📚 Allergic Rhinitis Lessons
The modern way to classify Allergic Rhinitis is the ARIA (Allergic Rhinitis and its Impact on Asthma) classification. We've moved away from just saying "seasonal" or "perennial" because many patients have symptoms year-round with seasonal peaks.
ARIA classifies it based on duration (Intermittent vs. Persistent) and severity (Mild vs. Moderate-Severe). Here is a quick breakdown:
| Feature | Intermittent | Persistent |
|---|---|---|
| Duration | < 4 days per week OR < 4 consecutive weeks | > 4 days per week AND > 4 consecutive weeks |
| Severity | Criteria |
|---|---|
| Mild | Normal sleep, no impairment of daily activities/work/school, no troublesome symptoms |
| Moderate-Severe | One or more of: Abnormal sleep, impairment of daily activities, troublesome symptoms |
Diagnosis is mostly clinical, based on a classic history of paroxysmal sneezing, watery rhinorrhea, and nasal itching. On examination, you'll see some very characteristic signs that are high-yield for your clinical exams:
- Allergic Shiners: Dark circles under the eyes due to venous congestion.
- Allergic Salute: Pushing the nose upward with the palm to relieve itching.
- Transverse Nasal Crease: A horizontal line across the lower third of the nose from all that "saluting."
- Dennie-Morgan Lines: Extra folds of skin under the lower eyelids.
Let me find an image showing these classic clinical signs for you.
These clinical signs are classic for "allergic facies" and are often seen in pediatric patients.
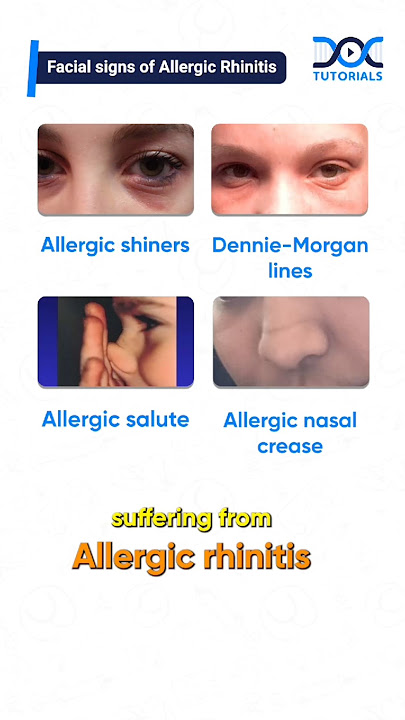
This image illustrates the classic facial signs: allergic shiners, Dennie-Morgan lines, the allergic salute, and the resulting nasal crease.
Now, for Management, the goal is to control symptoms and prevent complications like sinusitis or asthma exacerbations. The gold standard for treatment is Intranasal Corticosteroids (INS).
Let me show you a simplified management algorithm based on the ARIA guidelines.
The key takeaway for your exams is that Intranasal Steroids (INS) are the most effective single therapy for Allergic Rhinitis, especially for nasal congestion. For patients with co-existing asthma, Montelukast (LTRA) is a great choice.
If symptoms are refractory despite optimal medical management, Immunotherapy (SLIT or SCIT) is the only treatment that can potentially modify the disease course.
To help you lock in these concepts, would you like to try a quick word-grouping game to categorize symptoms, signs, and treatments?
Setting up chat...