Acute kidney injury: KDIGO staging, causes and fluid management
Acute kidney injury (AKI) is a massive topic for the UKMLA AKT, and getting the KDIGO staging down is essential because it often dictates how aggressively we manage these patients on the wards.
Here is the KDIGO staging criteria, which is based on either serum creatinine or urine output—whichever is worse!
| Stage | Serum Creatinine Criteria | Urine Output Criteria |
|---|---|---|
| Stage 1 | 1.5–1.9x baseline OR increase of $\ge$ 26.5 $\mu$mol/L within 48h | < 0.5 mL/kg/h for 6–12 hours |
| Stage 2 | 2.0–2.9x baseline | < 0.5 mL/kg/h for $\ge$ 12 hours |
| Stage 3 | $\ge$ 3.0x baseline OR increase to $\ge$ 354 $\mu$mol/L OR start of RRT | < 0.3 mL/kg/h for $\ge$ 24 hours OR Anuria for $\ge$ 12 hours |
When we think about the causes of AKI, it's easiest to break them down by where the "plumbing" issue is: Pre-renal (blood flow to the kidney), Renal/Intrinsic (the kidney tissue itself), and Post-renal (the drainage system).
- Pre-renal (approx. 60-70%): This is usually due to hypoperfusion. Think dehydration, sepsis (vasodilation), or heart failure.
- Renal/Intrinsic: Damage to the tubules (Acute Tubular Necrosis is the most common), the glomerulus (Glomerulonephritis), or the interstitium (Acute Interstitial Nephritis—often drug-induced).
- Post-renal: Obstruction! Kidney stones, BPH, or pelvic malignancies blocking the ureters or urethra.
Let me find a visual to help you map these out.
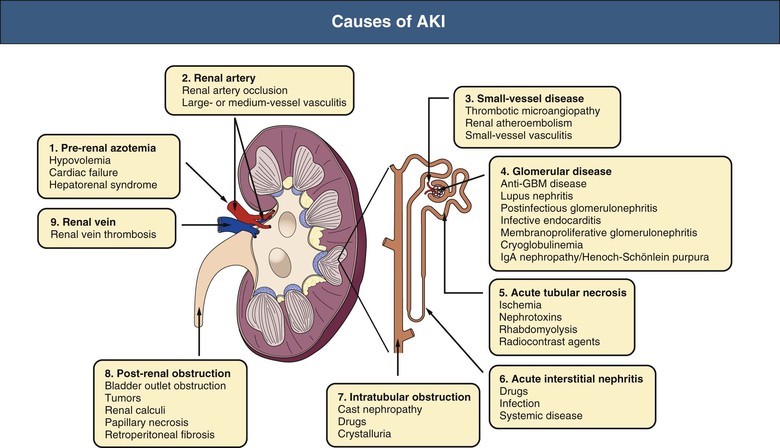
This diagram gives a great overview of how we categorize AKI. For your exams, remember that Acute Tubular Necrosis (ATN) is the most common intrinsic cause, often following a period of prolonged pre-renal hypoperfusion.
Fluid Management in AKI
Fluid management is a delicate balancing act. In the UK, we follow NICE guidelines (CG174) for intravenous fluid therapy.
- Assessment: Check the patient's fluid status (JVP, capillary refill, lung base crackles, peripheral edema).
- Fluid Resuscitation: If the patient is hypovolemic (e.g., Stage 1 or 2 AKI due to dehydration), give a bolus of crystalloid (like 0.9% Sodium Chloride or Hartmann's). Usually, 250–500 mL over less than 15 minutes.
- Maintenance: If they can't drink, they need maintenance fluids (approx. 25-30 mL/kg/day of water, with electrolytes).
- The Danger Zone: Be extremely careful with fluid overload. If the AKI is Stage 3 and the patient is anuric, giving more fluids will just lead to pulmonary edema. In these cases, we often restrict fluids and consider renal replacement therapy (dialysis).
Key Tip: Always review the "STOP" medications in AKI: S-NSAIDs, T-Toxic drugs (Gentamicin), O-Opiates (accumulation), P-Pills for BP (ACE inhibitors/ARBs/Diuretics).
Let me pull up some lessons and flashcards to help you lock this in for the AKT!
Those lessons will give you the deep dive you need for the AKT. To help you memorize the KDIGO criteria and the "STOP" drugs, I've pulled some flashcards for you to review.
Those flashcards should help you nail the pathophysiology and management steps. AKI is a classic exam topic because it tests your ability to interpret lab values, understand anatomy, and make safe clinical decisions about fluids and medications.
If you're feeling confident, we could try a quick Clinical Rounds case to see how you'd manage an AKI patient in a real-world scenario, or I can pull up some PYQs (Previous Year Questions) to see how this usually appears on the AKT. What do you think?
Setting up chat...