Addison's disease vs Cushing's syndrome: clinical features and investigation
Ah, the classic adrenal tug-of-war! Addison's and Cushing's are basically polar opposites when it comes to cortisol levels—one is a "not enough" problem, and the other is a "way too much" problem.
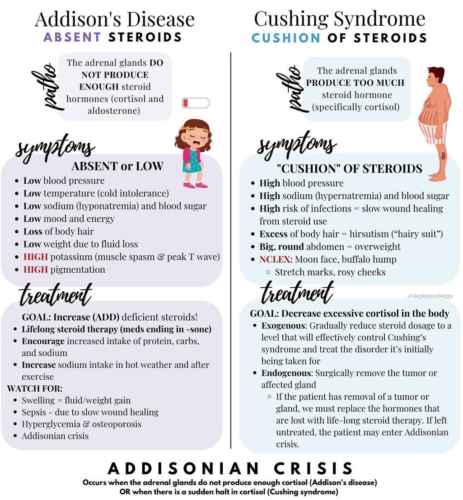
Since you're prepping for the UKMLA AKT, these are high-yield topics because they love to test the biochemical shifts and those classic "spot diagnosis" clinical features. Let me grab a visual for you that highlights the physical changes we see in these patients.
That infographic is a great summary of how these two present. In Addison's, you're looking for that "bronzed" look and low blood pressure, while Cushing's is all about the "C's": Central obesity, Collagen wasting (striae), and Calcium loss (osteoporosis).
Let me put this into a clear comparison table for you to make it easier to digest.
The visual really highlights the "opposite" nature of these conditions. To help you with your AKT revision, here's a breakdown of the clinical features and the high-yield investigations you'll need to know.
Clinical Features Comparison
| Feature | Addison's Disease (Primary Adrenal Insufficiency) | Cushing's Syndrome (Hypercortisolism) |
|---|---|---|
| Weight | Weight loss / Anorexia | Central obesity, "Moon face", "Buffalo hump" |
| Skin | Hyperpigmentation (palmar creases, scars, buccal mucosa) | Thin skin, easy bruising, purple striae |
| Blood Pressure | Hypotension (postural) | Hypertension |
| Mood/Energy | Lethargy, depression | Psychosis, insomnia, depression |
| Other | Salt craving, loss of pubic hair (in women) | Proximal muscle weakness, hirsutism, osteoporosis |
High-Yield Investigations
For the AKT, you need to know the "first-line" vs "gold standard" tests.
1. Addison's Disease
- Initial Bloods:
HyponatraemiaandHyperkalaemiaare the classic U&E findings. You might also see hypoglycemia. - Screening: 9 am Serum Cortisol (if <100 nmol/L, it's very likely; if >500 nmol/L, it's unlikely).
- Gold Standard: Short Synacthen Test (ACTH stimulation test). We give IM/IV tetracosactide and measure cortisol at 30 and 60 mins. A "fail" is a cortisol level that doesn't rise above
425-500 nmol/L. - ACTH Levels: High in primary adrenal insufficiency (Addison's) because the pituitary is screaming at the adrenals to work.
2. Cushing's Syndrome
- Initial Bloods:
Hypokalaemia(especially in ectopic ACTH) andHyperglycaemia. - Screening (Pick one):
- Overnight Dexamethasone Suppression Test (ODST): Give 1mg dex at midnight, check cortisol at 8 am. Normal people suppress; Cushing's patients don't.
- 24-hour Urinary Free Cortisol.
- Late-night Salivary Cortisol.
- Localization: Once you confirm Cushing's, you check ACTH to see if it's ACTH-dependent (Pituitary/Ectopic) or independent (Adrenal tumor).
Mnemonic: Addison's adds "Pigment" and "Potassium" (Hyperpigmentation and Hyperkalaemia)
I'll pull up some lessons and flashcards so you can lock this in!
📚 Adrenal Pathology Lessons
Those lessons cover the pathophysiology and the management in more detail, which is great for the AKT. To help you memorize the key diagnostic steps, I'll pull up some flashcards.
🗂️ Adrenal Flashcards
Tap to study 4 flashcards in the Oncourse app
Those flashcards are perfect for testing your recall on the diagnostic criteria. Remember, the AKT loves to throw a "distractor" at you—like a patient with high ACTH and hyperpigmentation, which points you straight to Primary Adrenal Insufficiency (Addison's).
If you're feeling confident with the theory, we could try a quick clinical case to see how you'd manage a patient presenting with these symptoms in a real-world scenario!
Setting up chat...