Acute upper GI bleed: Rockall score, resuscitation and endoscopy timing
Managing an acute upper gastrointestinal bleed (UGIB) is a classic "bread and butter" topic for the UKMLA AKT. It's all about rapid assessment, stabilization, and knowing exactly when to involve the endoscopists.
Resuscitation: The ABCDE Approach
In the UK, we follow the NICE (CG141) and BSG guidelines. Your first priority is always stabilization before diagnosis.
- A/B: Ensure the airway is protected (especially if there's massive hematemesis) and provide high-flow oxygen if needed.
- C (Circulation): This is where the heavy lifting happens.
- Access: Insert two large-bore (14G or 16G) peripheral cannulae.
- Fluids: Start warmed crystalloids if the patient is hypotensive or tachycardic.
- Transfusion: NICE recommends a restrictive strategy. Transfuse red blood cells if Hb < 70 g/L (target 70-90 g/L). If the patient has known cardiovascular disease, the threshold is slightly higher at Hb < 80 g/L.
- Platelets/FFP: Give platelets if the count is < 50 x 10⁹/L. Give FFP if the INR is > 1.5.
- Terlipressin and Antibiotics: If you suspect variceal bleeding (e.g., history of cirrhosis), start these before endoscopy.
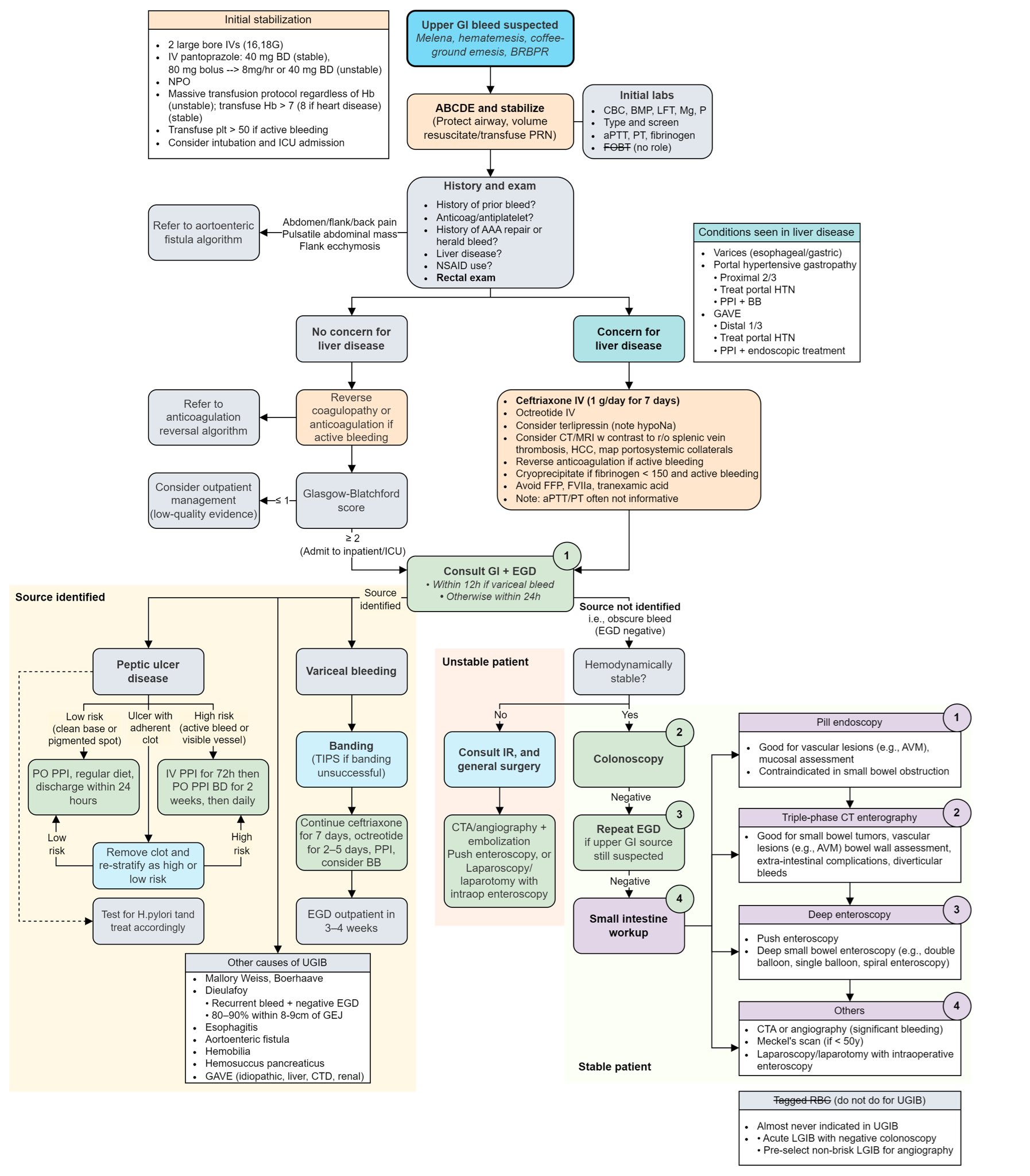
I'll pull up a clinical algorithm to help you visualize the management flow.
That flowchart gives a great overview of the clinical pathway. Let's look at that visually before we dive into the scoring systems.
Risk Scoring: Rockall vs. Glasgow-Blatchford
In the UK, you need to know two main scores. While you asked about the Rockall score, the Glasgow-Blatchford Score (GBS) is actually the one we use first in the ED.
- Glasgow-Blatchford Score (GBS): Used pre-endoscopy. It helps you decide if the patient needs to be admitted. A score of 0 is low risk, and these patients can often be managed as outpatients.
- Rockall Score: This is used to predict mortality. It has two parts:
- Pre-endoscopy Rockall: Based on age, shock (HR/BP), and comorbidities.
- Post-endoscopy Rockall: Adds the endoscopic diagnosis and "stigmata of recent hemorrhage" (like a visible vessel or a clot).
Endoscopy Timing
The timing of the OGD (Oesophago-Gastro-Duodenoscopy) is a common exam question:
- Unstable patients: Should have an endoscopy immediately after resuscitation.
- All other patients: Should have an endoscopy within 24 hours of admission.
I've put together a quick comparison table to help you keep the scores straight for your finals.
| Feature | Glasgow-Blatchford Score (GBS) | Rockall Score |
|---|---|---|
| When to use | Pre-endoscopy (at presentation) | Post-endoscopy (usually) |
| Primary Goal | Identifies who needs intervention/admission | Predicts risk of re-bleeding and mortality |
| Key Components | Urea, Hb, Systolic BP, HR, Melena, Syncope, Liver disease, Heart failure | Age, Shock (HR/BP), Comorbidities, Diagnosis, Evidence of bleeding |
| High-Yield Fact | A score of 0 = safe for discharge | A post-endoscopy score < 3 = low risk of death |
That table should help you distinguish between the two in a SBA (Single Best Answer) question.
One final high-yield tip for the AKT: Proton Pump Inhibitors (PPIs). NICE is very specific here—do not give a PPI before endoscopy for a non-variceal bleed, as it can mask the underlying cause. You only start high-dose IV PPIs after the endoscopy has confirmed a peptic ulcer with high-risk features.
If you want to dive deeper into the specific endoscopic treatments (like adrenaline injection vs. banding), I can pull up some detailed lessons for you.
📚 Upper GI Bleed Lessons
I've linked some high-yield lessons above that cover the surgical and medical management in more detail, including the specific steps for cirrhosis and variceal bleeds. Let me know if you'd like to try a few practice questions on this topic!
Setting up chat...