Acute MI management: reperfusion strategy, medications and complications
Managing an acute Myocardial Infarction (MI) is definitely one of those "must-know" topics for the USMLE. It’s all about speed and stabilizing the heart muscle before too much damage occurs.
Let's start by looking at some high-yield lessons that break down the management protocols and the pathophysiology behind them.
When a patient rolls into the ER with a suspected MI, we usually think of the mnemonic MONA-BASH for initial and long-term medical management.
1. Medications: The "MONA-BASH" Protocol
- Morphine: For pain relief (use with caution as it can mask symptoms).
- Oxygen: Only if $O_2$ saturation is $< 90%$.
- Nitrates: To reduce preload and coronary vasodilation (avoid in right ventricular MI!).
- Aspirin: 325 mg chewed immediately (antiplatelet).
- Beta-blockers: Reduce myocardial $O_2$ demand (avoid in heart failure or bradycardia).
- ACE inhibitors: Prevent cardiac remodeling.
- Statins: High-intensity (e.g., Atorvastatin 80mg) for plaque stabilization.
- Heparin: Anticoagulation (Unfractionated or LMWH).
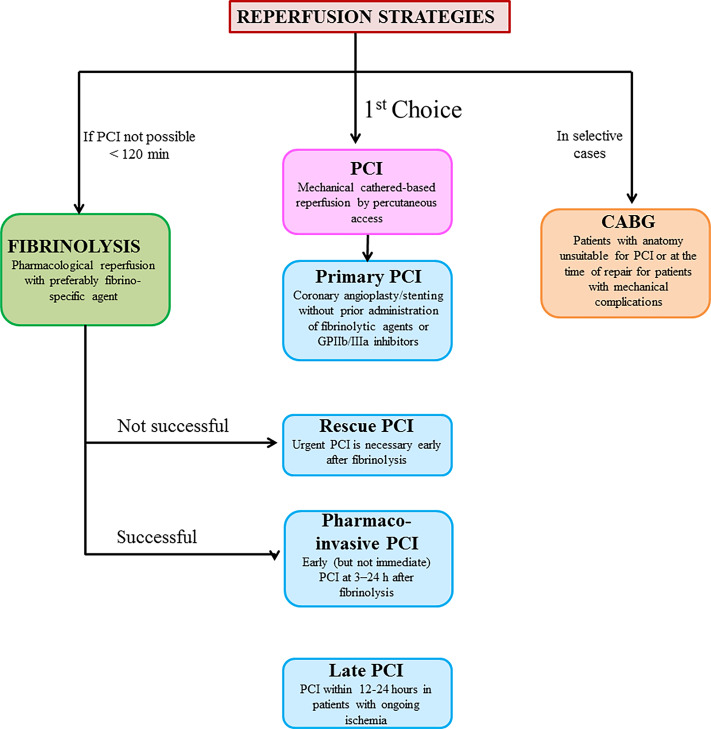
2. Reperfusion Strategy (The "Time is Muscle" Phase)
This depends entirely on whether you see ST-elevation (STEMI) or not (NSTEMI).
- STEMI: Requires immediate reperfusion.
- Percutaneous Coronary Intervention (PCI): The gold standard. Goal is "Door-to-Balloon" time < 90 minutes.
- Fibrinolytics (e.g., Alteplase): Used if PCI isn't available within 120 minutes. Goal is "Door-to-Needle" time < 30 minutes.
- NSTEMI: Usually managed with "MONA-BASH" and anticoagulation first, followed by a diagnostic catheterization within 24–48 hours.
I'll pull up a clinical algorithm to help you visualize the decision-making process for reperfusion.
The timing of reperfusion is critical, as shown in this management algorithm.
Finally, let's talk about complications. For the USMLE, you must know the timing of these events, as they often give you a "3 days post-MI" or "2 weeks post-MI" scenario.
| Timing | Complication | Key Clinical Sign |
|---|---|---|
| < 24 hours | Ventricular Arrhythmias (V-fib) | Most common cause of sudden death post-MI |
| 1 - 3 days | Post-infarction Pericarditis | Friction rub, pleuritic chest pain |
| 3 - 14 days | Free Wall Rupture | Cardiac tamponade (Beck's triad) |
| 3 - 14 days | Papillary Muscle Rupture | New holosystolic murmur (Mitral Regurgitation) |
| 3 - 14 days | Ventricular Septal Rupture | New holosystolic murmur (Left-to-right shunt) |
| > 2 weeks | Dressler Syndrome | Autoimmune pericarditis (fever, friction rub) |
| Months | Ventricular Aneurysm | Persistent ST elevation, risk of mural thrombus |
High-Yield Tip: If you see a patient with sudden hypotension and a new murmur 5 days after an MI, think Papillary Muscle Rupture (if it's Mitral Regurgitation) or VSR (if there's a step-up in $O_2$ in the right ventricle).
Would you like to test your knowledge on these complications with a quick quiz or maybe some flashcards?
Setting up chat...