Acute chest pain: differential diagnosis and emergency assessment pathway
Acute chest pain is one of the most common and high-stakes presentations you'll encounter, both in the ED and on your UKMLA AKT. The goal is always to "rule out the killers" first while systematically narrowing down the cause.
I've put together a breakdown of the key differentials you need to keep on your radar, categorized by system to help your clinical reasoning.
| System | Life-Threatening (The "Killers") | Common/Other Differentials |
|---|---|---|
| Cardiac | ACS (STEMI, NSTEMI, Unstable Angina), Aortic Dissection | Stable Angina, Pericarditis, Myocarditis |
| Respiratory | Tension Pneumothorax, Pulmonary Embolism (PE) | Pneumonia, Pleurisy, Simple Pneumothorax |
| Gastrointestinal | Oesophageal Rupture (Boerhaave's) | GORD, Oesophageal Spasm, Peptic Ulcer, Biliary Colic |
| Musculoskeletal | - | Costochondritis, Rib fracture, Muscle strain |
| Psychological | - | Anxiety / Panic Attack |
When a patient rolls in with acute chest pain, your assessment needs to be rapid and structured. In the UK, we strictly follow the ABCDE approach while simultaneously hunting for red flags like hemodynamic instability or "tearing" pain.
==The "Golden Rule": A 12-lead ECG should be performed and interpreted within 10 minutes of arrival for all patients with suspected ACS.==
Here is a simplified emergency assessment pathway to guide your initial management:
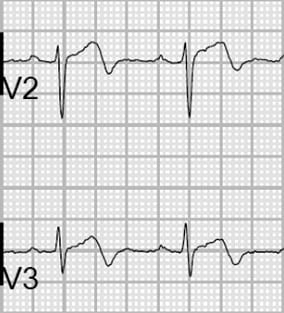
Recognizing the "killer" patterns on an ECG is a vital skill. For example, in a STEMI, you're looking for ST-segment elevation in two or more contiguous leads.
Let me find a clear visual for you that highlights some of these critical findings.
This ECG is a classic example of what we call "tombstoning" ST elevation, which is a sign of a massive acute myocardial infarction.
To really master this for your exams and clinical rotations, I've pulled some key lessons that dive deeper into the management of ACS, PE, and other critical chest pain causes.
📚 Chest Pain Mastery Lessons
These lessons cover everything from the specific red flags you need to ask about in your history to the latest management protocols for STEMI and aortic dissection.
Remember, for the AKT, they love testing the "next best step" in management, so pay close attention to the timing of ECGs and the use of risk scores like the Wells score for PE or the GRACE score for NSTEMI.
Let me know if you want to dive into any of these specific conditions or if you'd like to try a quick quiz to test your knowledge!
Setting up chat...