Acute care management principles for USMLE Step 3
Hey there! Diving into acute care management for Step 3 is a smart move—it's the bread and butter of the CCS (Computer-based Case Simulations) and a huge part of the multiple-choice section. Think of it as your "first 5 minutes" in the ER or ICU.
Let me pull up some high-yield lessons that break down these management protocols so you can see exactly how the exam expects you to prioritize.
📚 Acute Care Lessons
Those lessons are gold for understanding how to prioritize medications and distinguish between acute and chronic management—a classic Step 3 trap!
When you're faced with an acute case, your brain should automatically flip to the ABCDE assessment. It’s the universal language of emergency medicine. I'll grab a quick visual for you that outlines this primary survey, as it's the foundation for every "Emergency" or "Urgent" case you'll see.
This visual is a perfect reminder of the sequence you must follow for any unstable patient.
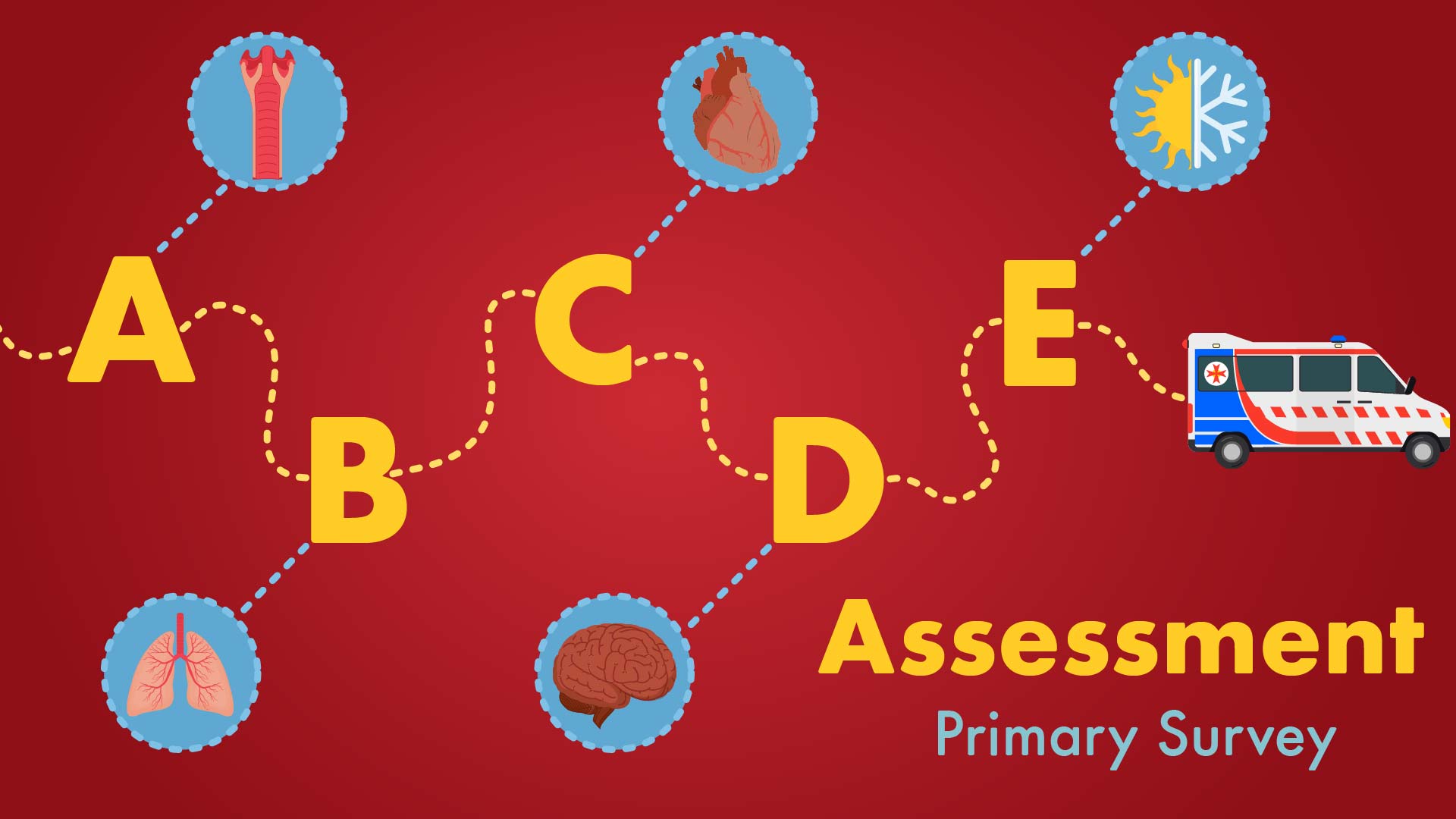
The ABCDE framework ensures that life-threatening conditions are addressed in order of their immediate impact on survival.
That ABCDE framework is your safety net. If you follow it, you'll never miss a critical step in a high-pressure scenario. For Step 3, especially the CCS cases, you need to be systematic.
Here’s how to break down the Acute Care Management Principles:
1. The "First 5 Minutes" (Stabilization)
Before you even think about a definitive diagnosis, you must stabilize the patient. In a CCS case, these are the orders you should place immediately for any acutely ill patient:
- Pulse Oximetry and Oxygen (if saturation is low or patient is in distress).
- Cardiac Monitor and ECG.
- IV Access (usually 2 large-bore IVs if the patient is unstable).
- Normal Saline or Lactated Ringer's (if hypotensive).
- Vital Signs (if not already provided).
Mnemonic: MOVIE Monitor, Oxygen, Vitals, IV access, ECG/Labs
2. Primary Survey (ABCDE)
- Airway: Is it patent? Do they need intubation? ==GCS < 8 = Intubate==.
- Breathing: Check breath sounds. Is there a tension pneumothorax?
- Circulation: Check pulses, BP, and capillary refill. Start fluids or vasopressors if needed.
- Disability: Check GCS and pupils. Don't forget a finger-stick glucose! ==Hypoglycemia can mimic a stroke==.
- Exposure: Undress the patient to look for hidden trauma or rashes, but keep them warm.
3. Diagnostic Workup (The "Big Six" Labs)
For almost every acute patient, you'll want these baseline labs:
- CBC (Infection, anemia).
- BMP/CMP (Electrolytes, renal function).
- PT/INR/PTT (Coagulation status).
- Troponin (If chest pain or elderly).
- Urinalysis (Infection, stones).
- CXR (Heart failure, pneumonia, PTX).
4. Management Prioritization
- Acute vs. Chronic: Always treat the acute problem first. If a patient has a COPD exacerbation and chronic hypertension, ==fix the breathing before you worry about the BP== (unless it's a hypertensive emergency).
- Empiric Therapy: Don't wait for cultures. If you suspect sepsis, start broad-spectrum antibiotics (e.g., Vancomycin + Ceftriaxone) immediately after drawing blood cultures.
5. Disposition
Once stabilized, decide where the patient goes:
- ICU: If they need vasopressors, mechanical ventilation, or frequent monitoring.
- Ward: If they are stable but need IV meds or further workup.
- Home: Only if the acute issue is resolved and they have a safe follow-up plan.
Would you like to try a quick Clinical Rounds case to see how you'd apply these principles in a real-time scenario? It's a great way to practice the prioritization we just talked about!
Setting up chat...