Acute asthma attack in A&E: assessment, severity grading and management
Managing an acute asthma attack in the A&E is a classic UKMLA AKT topic. Since you're prepping for the UK exams, we'll stick closely to the BTS/SIGN guidelines, which are the gold standard here.
It’s all about staying calm, grading the severity quickly, and hitting them with the "O SHIT" treatment (more on that mnemonic in a second!).
1. Assessment & Severity Grading
The first thing you need to do is figure out how worried you should be. We grade these into Moderate, Severe, and Life-threatening.
| Feature | Moderate | Acute Severe | Life-Threatening |
|---|---|---|---|
| PEFR | 50-75% predicted | 33-50% predicted | < 33% predicted |
| Respiratory Rate | < 25/min | $\ge$ 25/min | - |
| Heart Rate | < 110 bpm | $\ge$ 110 bpm | - |
| Speech | Normal | Cannot complete sentences | - |
| Other Signs | - | - | 33-92-CHEST (see below) |
Mnemonic: 33-92-CHEST (Life-Threatening Signs)
- 33: PEFR < 33%
- 92: SpO2 < 92%
- C: Cyanosis / Confusion
- H: Hypotension
- E: Exhaustion / Feeble respiratory effort
- S: Silent chest
- T: Tachyarrhythmia (or bradycardia)
2. Management (The "O SHIT!" Mnemonic)
This is the standard escalation of treatment in the A&E:
- O - Oxygen: Aim for sats of 94-98%.
- S - Salbutamol: 5mg nebulised (driven by oxygen).
- H - Hydrocortisone (IV) or Prednisolone (Oral): 40-50mg prednisolone is standard. Continue for at least 5 days.
- I - Ipratropium bromide: 0.5mg nebulised (add this for severe or life-threatening cases).
- T - Theophylline (Aminophylline): Usually an ICU/Senior decision if the patient isn't responding.
- ! - Magnesium Sulphate: 1.2–2g IV infusion over 20 mins (for severe/life-threatening cases).
3. When to refer to ICU?
If they have a "Normal" pCO2 on an ABG, that is a massive red flag. In an asthma attack, they should be hyperventilating (low pCO2). A normal or rising pCO2 means they are tiring out and might need intubation.
I'll pull up some high-yield lessons and a flowchart to help you visualize the management pathway.
📚 Asthma Management Lessons
I've found a great management algorithm that covers the step-up approach, which is vital for both acute and chronic management.
For the acute setting, remember that the "Life-Threatening" category is the one that usually requires an immediate call to the ICU/Anaesthetics team.
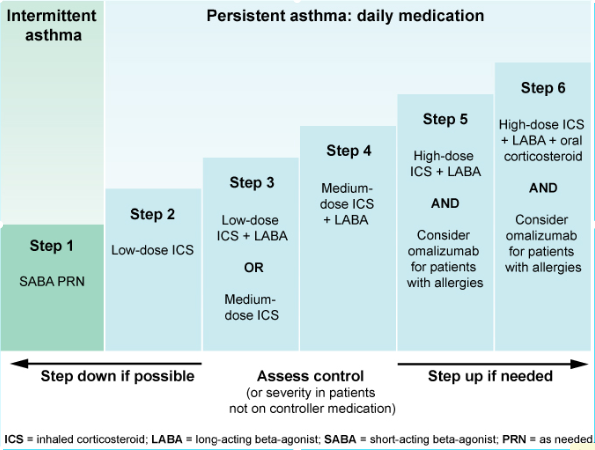
This algorithm shows the stepped care approach. In an acute A&E presentation, you are essentially jumping to the highest steps (Step 5/6) with systemic steroids and nebulised bronchodilators.
Discharge Criteria (High Yield for AKT)
Before you send them home, they must meet these BTS criteria:
- Stable on discharge medication (no nebs for 12-24 hours).
- PEFR > 75% of best or predicted.
- Inhaler technique checked and a written asthma action plan provided.
- GP follow-up within 2 working days.
- Respiratory clinic follow-up within 4 weeks.
Would you like to try a few practice questions on this to see how they frame it in the exam?
Setting up chat...