Acute coronary syndrome: STEMI vs NSTEMI diagnosis and management
Oh, Acute Coronary Syndrome (ACS)! This is bread-and-butter cardiology for the USMLE. Understanding the fork in the road between STEMI and NSTEMI is absolutely vital because it dictates how fast you need to move to save that myocardium.
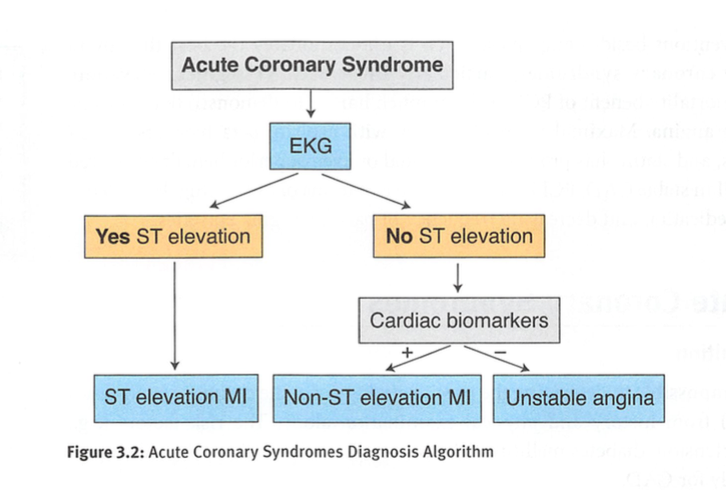
The primary distinction starts with the ECG and is confirmed by cardiac biomarkers. In a STEMI, you've got a complete coronary artery occlusion, whereas in NSTEMI (and Unstable Angina), the occlusion is usually subtotal or transient.
I've put together a quick comparison table to help you keep the diagnostic criteria straight.
| Feature | STEMI | NSTEMI |
|---|---|---|
| Pathophysiology | Complete occlusion (Transmural ischemia) | Subtotal occlusion (Subendocardial ischemia) |
| ECG Findings | ST-elevation in $\ge$ 2 contiguous leads; New LBBB | ST-depression, T-wave inversion, or non-specific changes |
| Cardiac Biomarkers | Elevated (Troponin I/T) | Elevated (Troponin I/T) |
| Urgency | Immediate reperfusion required ("Time is Muscle") | Urgent but usually not immediate (risk-stratified) |
When it comes to management, the mantra for STEMI is "Time is Muscle." You need to open that vessel immediately. The goal is Percutaneous Coronary Intervention (PCI) within 90 minutes (door-to-balloon time). If you're at a facility without PCI and can't transfer the patient quickly, fibrinolysis should be started within 30 minutes.
For NSTEMI, the approach is more about stabilization and risk stratification. We use the MONA-BASH mnemonic for initial medical therapy:
- Morphine (for refractory pain)
- Oxygen (if $O_2$ sat < 90%)
- Nitrates (vasodilation)
- Aspirin (immediate 325mg chewable)
- Beta-blockers (reduce $O_2$ demand)
- ACE inhibitors (long-term remodeling)
- Statins (high-intensity)
- Heparin (anticoagulation)
Let me find a visual aid that shows the diagnostic algorithm to make this even clearer.
This flowchart perfectly summarizes the diagnostic pathway we just discussed. It's a great mental map for when you're in the ED or answering a USMLE question.
To dive deeper into the specifics of each condition, I've pulled up some high-yield lessons for you.
📚 ACS Lessons
Those lessons cover the nitty-gritty of the management protocols. To help you lock in these facts, let's look at some flashcards.
Those flashcards are perfect for quick recall.
One last high-yield tip for your exams: Never wait for troponin results to treat a STEMI. If the ECG shows ST-elevation in a patient with classic chest pain, you activate the cath lab immediately. Troponins take time to rise (usually 3-6 hours), and in a STEMI, every minute counts!
If you're feeling confident, we could try a quick quiz or even a clinical case to see how you'd handle a patient in the ER. Just let me know!
Setting up chat...