Acute coronary syndromes: STEMI vs NSTEMI, troponin and management
Acute Coronary Syndrome (ACS) is a high-yield topic for the AKT, and it's essentially an umbrella term for three conditions: STEMI, NSTEMI, and Unstable Angina. The main goal is to distinguish between them quickly so you can start the right management pathway.
I'll pull up some of our best lessons on ACS to give you a solid foundation for your revision.
📚 ACS Lessons
The key to differentiating these is a combination of the ECG and cardiac troponins.
- STEMI: You'll see ST-elevation or a new Left Bundle Branch Block (LBBB) on the ECG. This indicates a complete coronary artery occlusion.
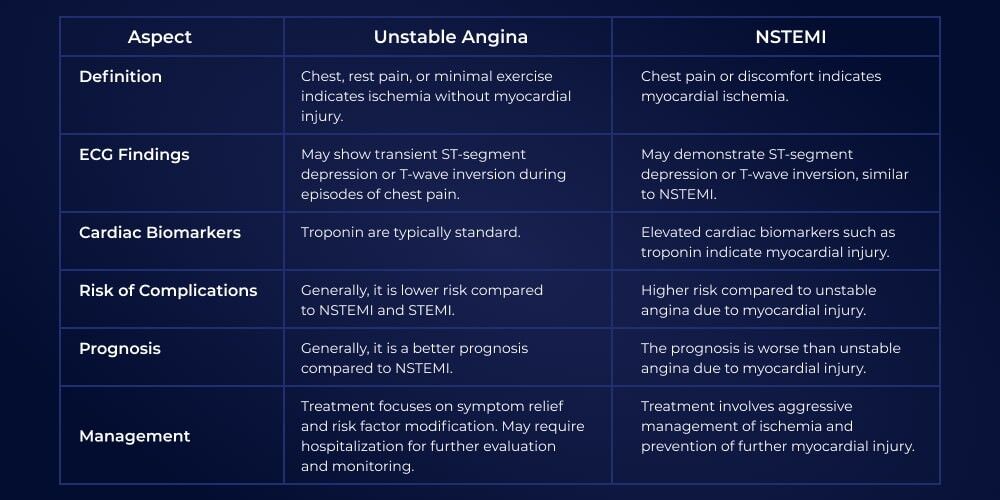
- NSTEMI: The ECG might show ST-depression, T-wave inversion, or even be normal, but the troponin will be elevated, indicating myocardial necrosis.
- Unstable Angina: Similar ECG changes to NSTEMI (or normal), but the troponin remains normal.
I'll find a clear comparison table to help you visualize these differences.
Management pathways differ significantly based on the type of ACS:
STEMI Management (The "Time is Muscle" Pathway)
- Immediate: Aspirin 300mg, Morphine (+ Metoclopramide), and GTN. Oxygen is only given if $SpO_2 < 94%$.
- Reperfusion:
- Primary PCI (pPCI) is the gold standard if it can be performed within 120 minutes of when fibrinolysis could have been given.
- Thrombolysis is used if pPCI is not available within that window.
- Dual Antiplatelet Therapy (DAPT): Aspirin + a second agent (usually Ticagrelor).
NSTEMI/Unstable Angina Management (The "Risk Stratification" Pathway)
- Initial: Aspirin 300mg and Fondaparinux (unless immediate PCI is planned or there's a high bleeding risk).
- Risk Assessment: Use the GRACE score to calculate 6-month mortality risk.
- High risk (GRACE >3%): Offer coronary angiography within 72 hours.
- Very high risk (unstable): Immediate angiography within 2 hours.
- DAPT: Aspirin + Ticagrelor (or Clopidogrel if bleeding risk is high).
The Role of Troponin
Troponin is highly specific for myocardial damage. In the UK, we typically use high-sensitivity troponin (hs-cTn).
- A diagnosis of MI requires a rise and/or fall of troponin levels with at least one value above the 99th percentile, alongside clinical evidence of ischemia (like chest pain or ECG changes).
- NICE recommends a rapid sampling protocol (e.g., at 0 and 3 hours) to rule in or rule out NSTEMI.
Would you like to try some practice questions to see how this shows up in the AKT?
✍️ ACS Practice Quiz
Tap to practice questions in the Oncourse app
I've set up a quiz for you with 10 questions focused on ACS diagnosis and management—it's a great way to test your understanding of the GRACE score and reperfusion windows.
If you have any specific questions about the medications used (like why we use Fondaparinux over Heparin in NSTEMI) or want to see a flowchart for the management algorithm, just let me know!
Setting up chat...