Acne vulgaris: pathogenesis, grading and stepwise treatment
Acne vulgaris is basically the "rite of passage" that almost every teenager (and many adults) goes through. It's a chronic inflammatory disease of the pilosebaceous unit.
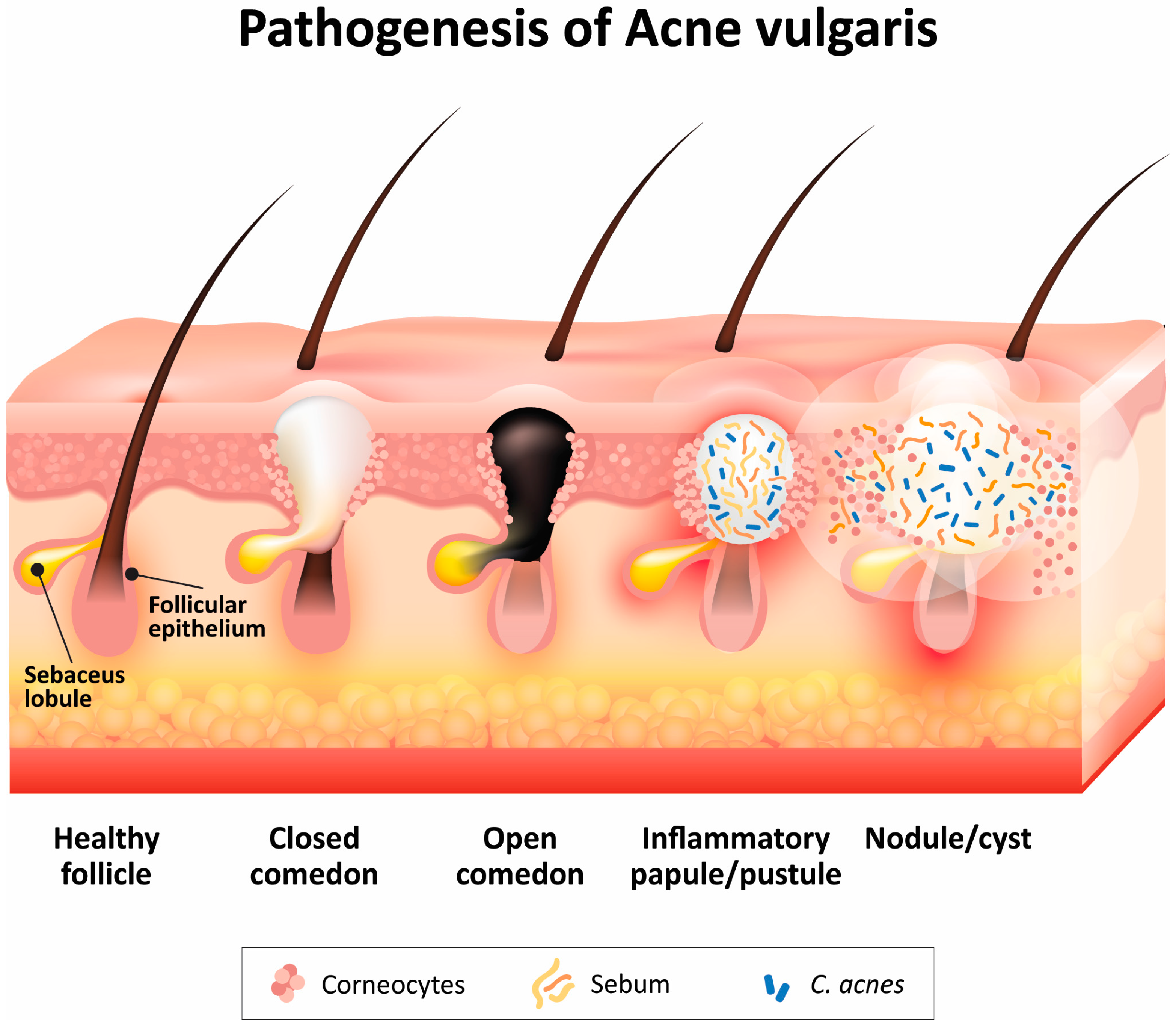
To understand how to treat it, we first have to look at the "four horsemen" of its pathogenesis. Let me find a good diagram to show you exactly how these factors interact to create those pesky breakouts.
The pathogenesis involves four key steps:
- Follicular Hyperkeratinization: Dead skin cells plug the follicle, forming a "microcomedone."
- Increased Sebum Production: Androgens stimulate sebaceous glands to pump out more oil.
- Colonization by Cutibacterium acnes: This bacterium loves sebum and thrives in the plugged follicle.
- Inflammation: The body's immune response to the bacteria and sebum leads to redness and swelling.
Now, let's look at how we grade acne clinically, as this determines our treatment strategy.
| Grade | Clinical Features | Primary Lesions |
|---|---|---|
| Grade 1 (Mild) | Non-inflammatory | Comedones (Open/Blackheads & Closed/Whiteheads) |
| Grade 2 (Moderate) | Mildly inflammatory | Papules + Comedones |
| Grade 3 (Severe) | Inflammatory | Pustules + Papules + Comedones |
| Grade 4 (Very Severe) | Severely inflammatory | Nodules, Cysts, and Scarring |
Once we've graded the acne, we follow a stepwise approach to treatment. Here's how we typically manage it:
Stepwise Treatment Strategy
-
Mild Acne (Grade 1)
- First-line: Topical Retinoids (e.g., Adapalene, Tretinoin) are the cornerstone.
- Add-on: Benzoyl Peroxide (BPO) to target C. acnes and prevent antibiotic resistance.
- Pro-tip: Apply retinoids at night because they're photolabile (break down in sunlight).
-
Moderate Acne (Grade 2-3)
- Topical Combo: Retinoid + BPO + Topical Antibiotic (e.g., Clindamycin).
- Oral Antibiotics: If topicals aren't enough, we add oral Doxycycline or Minocycline (usually for 3 months max).
- Note: Never use topical antibiotics alone; always pair them with BPO to avoid resistance!
-
Severe/Nodulocystic Acne (Grade 4)
- Oral Isotretinoin: This is the "big gun." It's the only drug that targets all four pathogenic factors.
- Safety: It's highly teratogenic, so female patients must be on strict contraception (the iPLEDGE program in the US).
High-Yield Fact: Benzoyl Peroxide is famous for bleaching your favorite pillowcases and towels—warn your patients!
Let me pull up some lessons and flashcards so you can lock this in for your exams.
📚 Acne Vulgaris Lessons
Those lessons cover the management and clinical types in detail. Before we wrap up with some flashcards, keep an eye out for these two severe variants that often pop up in exams:
- Acne Fulminans: Sudden onset of severe acne with systemic symptoms (fever, bone pain, high WBC). Treatment requires oral steroids before starting Isotretinoin.
- Acne Conglobata: A chronic, severe form with interconnected cysts and sinuses, but without the systemic symptoms of Fulminans.
Ready to test your memory? Here are some flashcards for you.
🗂️ Acne Vulgaris Flashcards
Tap to study 13 flashcards in the Oncourse app
Those flashcards should help you nail the key points on pathogenesis and side effects.
Acne is a high-yield topic because it's so common in clinical practice and exams. If you're feeling confident, we could try a quick quiz to see how you handle some clinical scenarios, or I can help you with any other dermatology doubts!
Setting up chat...