Acid-base balance: disorders, compensation and ABG interpretation
Acid-base balance is one of those topics that feels like a math test in the middle of a medical exam, but once you get the rhythm down, it's actually quite logical! It's all about keeping that pH in the tight window of 7.35 to 7.45.
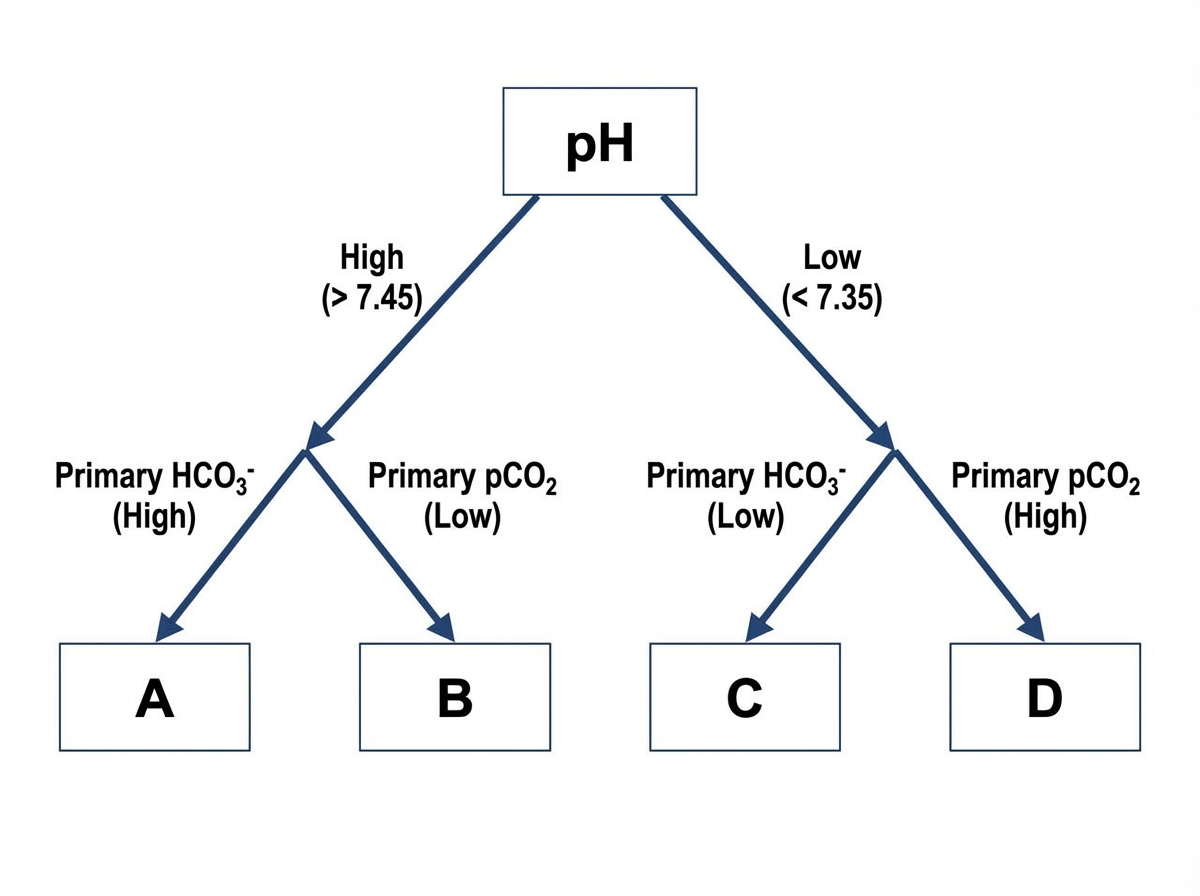
To help you visualize the diagnostic process, I'm going to find a clear flowchart for ABG interpretation.
That flowchart is a great starting point. Let's get it on your screen so we can walk through the steps together.
To master ABG interpretation, you just need to follow these three steps every single time:
- Check the pH: Is it low (< 7.35 = Acidosis) or high (> 7.45 = Alkalosis)?
- Find the Primary Cause:
- If the $pCO_2$ is moving in the opposite direction of the pH (e.g., low pH, high $pCO_2$), it's Respiratory.
- If the $HCO_3^-$ is moving in the same direction as the pH (e.g., low pH, low $HCO_3^-$), it's Metabolic.
- Assess Compensation: Is the "other" system trying to fix the pH? If the pH is back in the normal range, it's fully compensated. If it's still abnormal but the other value is moving to help, it's partially compensated.
Here is a quick reference table for the expected compensation in each primary disorder:
| Primary Disorder | Primary Change | Expected Compensation |
|---|---|---|
| Metabolic Acidosis | $\downarrow HCO_3^-$ | $\downarrow pCO_2$ (Winters' Formula: $1.5 \times HCO_3^- + 8 \pm 2$) |
| Metabolic Alkalosis | $\uparrow HCO_3^-$ | $\uparrow pCO_2$ (0.7 mmHg increase for every 1 mEq/L $\uparrow HCO_3^-$) |
| Respiratory Acidosis | $\uparrow pCO_2$ | $\uparrow HCO_3^-$ (Acute: 1 per 10; Chronic: 3.5 per 10 $\uparrow pCO_2$) |
| Respiratory Alkalosis | $\downarrow pCO_2$ | $\downarrow HCO_3^-$ (Acute: 2 per 10; Chronic: 5 per 10 $\downarrow pCO_2$) |
That table is your best friend for USMLE questions! If the measured $pCO_2$ is higher than Winters' formula predicts, you've got a concomitant respiratory acidosis. If it's lower, you've got a concomitant respiratory alkalosis.
To dive deeper into the specific causes (like MUDPILES for high anion gap metabolic acidosis), I've pulled up some high-yield lessons for you.
📚 Acid-Base Balance Lessons
Those lessons will give you the full breakdown of the clinical scenarios you'll see on the wards. To help you lock in those compensation rules and the "MUDPILES" mnemonic, I've also found some flashcards for you.
🗂️ Acid-Base Flashcards
Tap to study 20 flashcards in the Oncourse app
You've got the tools now to tackle any ABG that comes your way! Remember, the key is to be systematic: pH first, then the primary driver, then the compensation.
If you want to test how well you can categorize different clinical scenarios into these disorders, we could play a quick game of Synapses. It's a great way to see if you can group things like "Diarrhea," "Vomiting," and "COPD" into their correct acid-base categories. Want to give it a shot?
Setting up chat...