Abnormal uterine bleeding: causes, investigation and management by age
Abnormal Uterine Bleeding (AUB) is one of those bread-and-butter topics that you'll see everywhere—from your GP rotations to the AKT. It’s a bit of a catch-all term for any bleeding that doesn't fit the "normal" menstrual cycle pattern.
To keep things organized, we usually use the PALM-COEIN acronym developed by FIGO. It helps distinguish between structural and non-structural causes. Let me pull up a quick reference table for you!
| Category | Cause | Description |
|---|---|---|
| P | Polyps | Small growths in the endometrial lining |
| A | Adenomyosis | Endometrial tissue growing into the uterine muscle |
| L | Leiomyoma | Uterine fibroids (very common!) |
| M | Malignancy | Endometrial hyperplasia or cancer |
| C | Coagulopathy | Bleeding disorders (e.g., von Willebrand disease) |
| O | Ovulatory dysfunction | PCOS, thyroid issues, or stress |
| E | Endometrial | Primary disorders of endometrial local haemostasis |
| I | Iatrogenic | Medications (anticoagulants, copper IUD) |
| N | Not yet classified | Rare or unique causes |
The "why" behind the bleeding changes a lot depending on how old the patient is. It's all about where they are in their reproductive journey. Here’s how we usually break it down for the AKT:
1. Adolescents (Post-menarche)
- Most Common Cause: Anovulation due to an immature Hypothalamic-Pituitary-Ovarian (HPO) axis. It can take a year or two for cycles to become regular.
- Don't Forget: Coagulopathies (like von Willebrand disease) often present with heavy bleeding right from the first period.
2. Reproductive Age (20s to 40s)
- Pregnancy: ==Always exclude pregnancy first!== This is the golden rule of gynaecology.
- Structural: Fibroids (Leiomyomas), Polyps, and Adenomyosis.
- Hormonal: Polycystic Ovary Syndrome (PCOS) or thyroid dysfunction.
- Infection: Pelvic Inflammatory Disease (PID) or STIs.
3. Perimenopausal (Late 40s to early 50s)
- Anovulation: As the ovaries run out of eggs, cycles become irregular and often heavier.
- Malignancy Risk: This is where we start worrying more about Endometrial Hyperplasia or Endometrial Cancer.
4. Postmenopausal
- Most Common Cause: Atrophic Vaginitis (thinning of the lining due to low estrogen).
- Red Flag: Endometrial Cancer must be ruled out in every case of postmenopausal bleeding (PMB).
I'll find a good visual to help you map out the diagnostic approach for these patients.
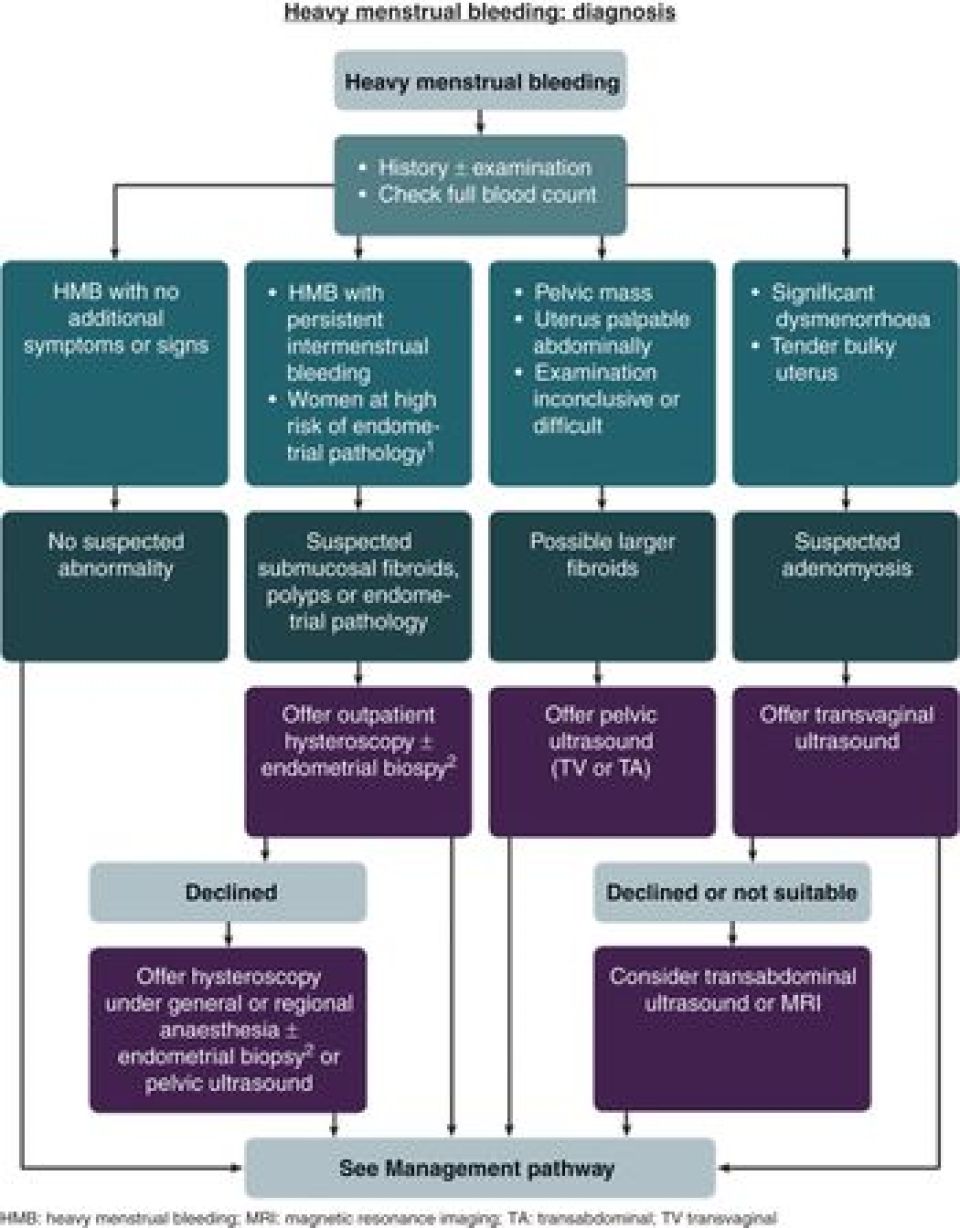
This diagnostic flowchart illustrates the systematic evaluation for heavy menstrual bleeding (HMB). It starts with history, physical examination, and full blood count, then branches based on symptoms like intermenstrual bleeding or suspected pelvic masses.
Once you've identified the likely cause, you'll need to confirm it with the right tests. For the AKT, remember that NICE guidelines are your best friend here.
Investigations: The Step-by-Step Approach
- Pregnancy Test: ==Mandatory for all women of reproductive age.==
- Full Blood Count (FBC): To check for iron-deficiency anaemia (very common with HMB).
- Coagulation Screen: Only if the patient has had heavy periods since menarche or a family history of bleeding disorders.
- Transvaginal Ultrasound (TVUS): The first-line imaging for structural issues like fibroids or adenomyosis.
- Endometrial Biopsy/Hysteroscopy: Required if:
- The patient is >45 years old.
- There is persistent intermenstrual bleeding.
- The endometrial thickness is >4mm on TVUS in a postmenopausal woman.
Management: The NICE Ladder
The goal is to reduce blood loss and improve quality of life.
- 1st Line: Levonorgestrel-releasing Intrauterine System (LNG-IUS), like the Mirena coil. It’s the most effective medical treatment.
- 2nd Line (if LNG-IUS is declined or unsuitable):
- Tranexamic acid: Non-hormonal, taken only during the period (antifibrinolytic).
- Mefenamic acid: An NSAID that also helps with dysmenorrhoea (pain).
- Combined Oral Contraceptive Pill (COCP): Good if they also want contraception.
- 3rd Line: Oral progestogens (like Norethisterone) or injected progestogens.
- Surgical Options: If medical management fails, consider Endometrial Ablation, Myomectomy (for fibroids), or Hysterectomy as a last resort.
I'll pull up some high-yield lessons on this so you can dive deeper into the specifics of each management option.
📚 AUB High-Yield Lessons
I've pulled up some high-yield lessons that cover the specifics of AUB, fibroids, and endometrial cancer—the big three you'll need for the AKT.
AUB is one of those topics where the management depends heavily on the patient's age and their future fertility plans. For example, a 25-year-old with fibroids who wants children will be managed very differently from a 52-year-old with the same issue!
Would you like to test your knowledge with a quick game to see if you can categorize these causes and treatments correctly? I can set up a Synapses game for you!
Setting up chat...