Abdominal pain in primary care: systematic assessment and red flag approach
Abdominal pain is one of those classic "bread and butter" topics in primary care, but it can be a real diagnostic challenge because almost anything from the chest to the pelvis can be the culprit! For the UKMLA AKT, the goal is to quickly differentiate between benign, self-limiting conditions and the "must-not-miss" surgical or medical emergencies.
Let's start by looking at some key lessons that break down the systematic approach to abdominal pain.
📚 Abdominal Pain Lessons
When you're in the GP surgery, your assessment needs to be efficient. I like to think of it as a funnel: start broad with the history, then narrow it down with the physical exam and red flags.
1. The Systematic History (SOCRATES)
The history is where you'll get 80% of your diagnosis. Use the SOCRATES acronym, but pay special attention to:
- Onset: Sudden (perforation, torsion, vascular) vs. gradual (inflammatory).
- Associated Symptoms: Fever, vomiting, change in bowel habit, urinary symptoms, or gynae history (always ask about the Last Menstrual Period!).
- Extra-abdominal causes: Don't forget that an inferior MI, pneumonia, or DKA can all present as abdominal pain.
2. Physical Examination
- Inspection: Scars (previous surgery = risk of obstruction), distension, or visible pulsations.
- Palpation: Start away from the pain. Look for guarding (voluntary) vs. rigidity (involuntary/peritonitis) and rebound tenderness.
- Special Tests: Murphy’s sign (cholecystitis), Rovsing’s sign (appendicitis).
- Don't forget: Check the hernial orifices and consider a PR or PV exam if the history points that way.
3. Red Flags (The "Must-Not-Miss")
These are the features that should make you consider an urgent referral or admission:
==Abdominal Pain Red Flags==
- Hemodynamic instability: Tachycardia, hypotension (think AAA or ectopic pregnancy).
- Signs of peritonitis: Rigidity, guarding, "pain with every bump in the road."
- Systemic upset: High fever, rigors, or jaundice.
- Suspected Cancer (NICE NG12): Unintentional weight loss, iron-deficiency anemia, or a palpable mass.
- Bowel Obstruction: Absolute constipation (no flatus), faeculent vomiting, and tinkling bowel sounds.
To help you visualize the differential diagnoses based on where the patient is pointing, let me pull up a helpful diagram and a comparison table.
This diagram is a great visual summary of how we categorize abdominal pain by quadrant. It's a high-yield way to organize your differential diagnosis for the AKT.
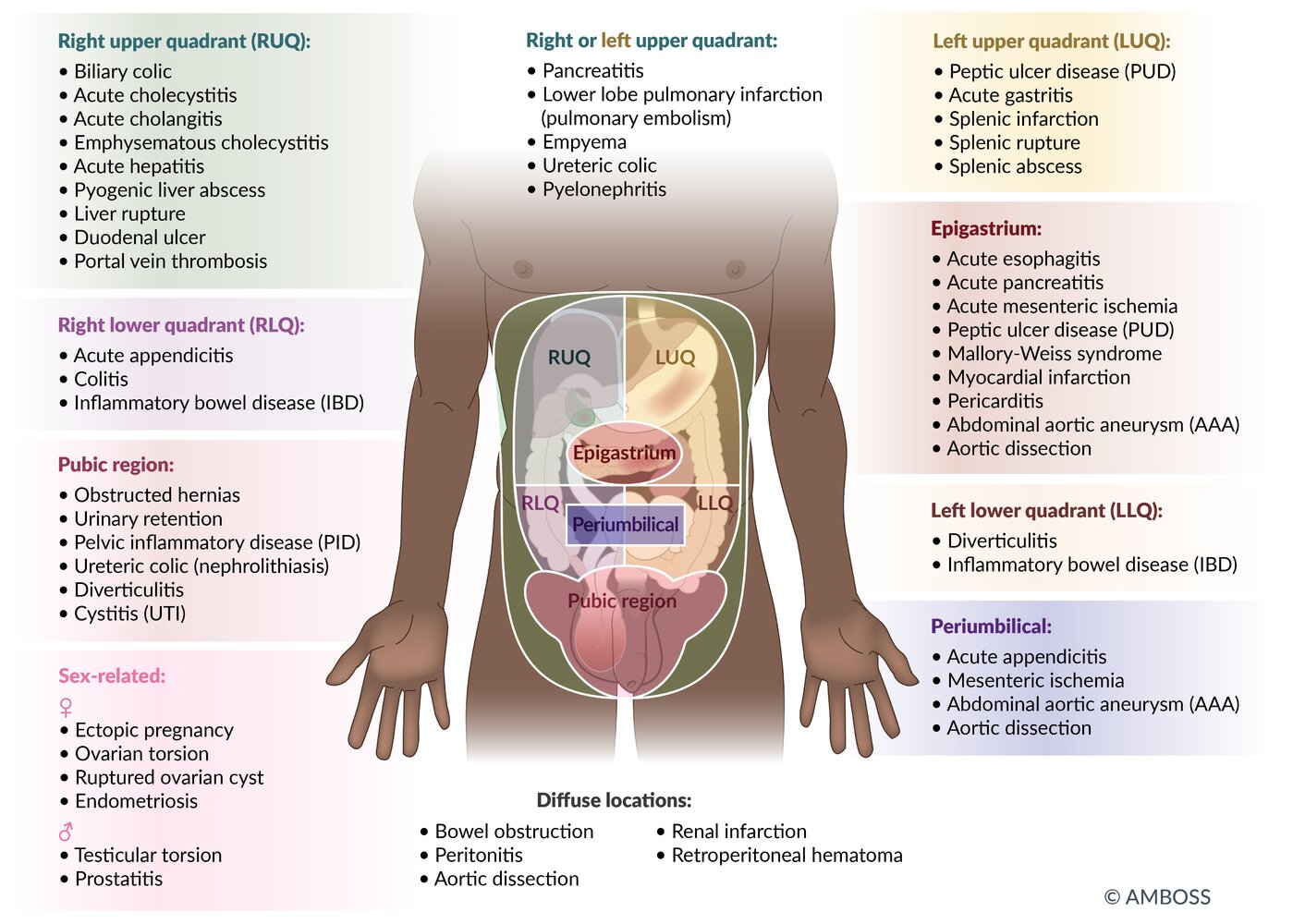
Differential Diagnosis by Quadrant
| Quadrant | Common Differentials |
|---|---|
| Right Upper (RUQ) | Biliary colic, Cholecystitis, Hepatitis, Pneumonia (referred) |
| Epigastric | GORD, Peptic Ulcer Disease, Gastritis, Pancreatitis, MI (referred) |
| Left Upper (LUQ) | Splenic infarct/rupture, Gastritis, Pneumonia (referred) |
| Periumbilical | Early Appendicitis, Small Bowel Obstruction, AAA |
| Right Lower (RLQ) | Appendicitis, Ectopic Pregnancy, Ovarian Torsion, Crohn's, Renal Colic |
| Left Lower (LLQ) | Diverticulitis, Ectopic Pregnancy, Ovarian Torsion, Renal Colic |
| Suprapubic | Cystitis, Urinary Retention, PID, Endometriosis |
To wrap up your systematic assessment, you'll need to consider your initial investigations. In primary care, these are often "rule-out" tests:
- Bedside: Urine dipstick (UTI/renal colic), Pregnancy test (mandatory in any woman of childbearing age!), and basic obs (BP, HR, Temp).
- Bloods: FBC (infection/anemia), CRP (inflammation), LFTs (biliary), Amylase (pancreatitis), and U&Es (dehydration/renal function).
- Imaging: In GP, you might order a non-urgent Ultrasound (USS) for suspected gallstones or a CT for suspected cancer (via the 2-week wait pathway).
Safety Netting is the final, vital step. If you're sending a patient home, they need to know exactly what to look for (e.g., "If the pain moves to the right lower side or you start vomiting, you must go to A&E").
Does that help clarify the approach, or would you like to dive deeper into a specific differential, like appendicitis or diverticulitis?
Setting up chat...