Acute abdominal emergencies: appendicitis, bowel obstruction, perforation
Dealing with an acute abdomen is like being a medical detective—you have to figure out if the patient needs a surgeon right now or if it's something that can be managed medically. Appendicitis, bowel obstruction, and perforation are the "big three" surgical emergencies you'll see constantly in the ER.
Let's break down the high-yield clinical features and management for each of these.
1. Acute Appendicitis
This is the most common reason for emergency abdominal surgery. The classic presentation is a "migratory" pain pattern.
- Clinical Presentation: Starts as vague periumbilical pain (visceral) that later localizes to the Right Lower Quadrant (RLQ) at McBurney’s point (somatic).
- Key Signs:
- Rovsing Sign: Pain in RLQ with palpation of the LLQ.
- Psoas Sign: Pain on passive extension of the right hip.
- Obturator Sign: Pain on internal rotation of the flexed right hip.
- Diagnosis: In adults, a CT scan with IV contrast is the gold standard. In kids and pregnant women, we start with Ultrasound.
2. Small Bowel Obstruction (SBO)
Most SBOs are caused by post-surgical adhesions, while large bowel obstructions are more often due to malignancy.
- Clinical Triad:
- Colicky abdominal pain
- Nausea and vomiting (bilious if the obstruction is high)
- Abdominal distension and inability to pass flatus (obstipation).
- Physical Exam: You might hear high-pitched "tinkling" bowel sounds early on, which go silent later.
- Imaging: An abdominal X-ray will show dilated loops of bowel and air-fluid levels.
3. Gastrointestinal Perforation
This is a true "surgical "catastrophe." Whether it's from a peptic ulcer, diverticulitis, or trauma, the result is peritonitis.
- Clinical Presentation: Sudden, "thunderclap" onset of severe, generalized abdominal pain.
- Physical Exam: The classic "board-like" rigid abdomen with guarding and rebound tenderness.
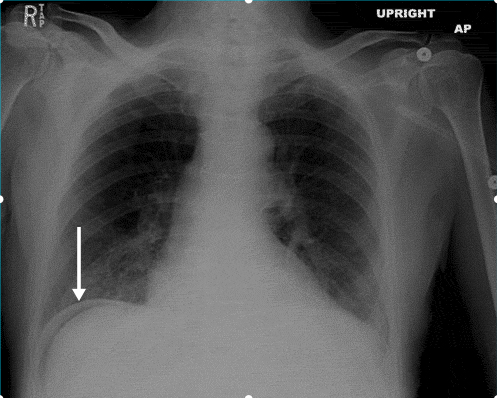
- Imaging: An upright chest X-ray is your best friend here—look for pneumoperitoneum (free air under the diaphragm).
I'll pull up some high-yield lessons and a diagnostic algorithm to help you visualize how to differentiate these in a clinical setting.
📚 Acute Abdomen Lessons
That upright X-ray is a classic "spot diagnosis" for perforation. When you see that crescent of air under the diaphragm, it's a surgical emergency.
To help you keep these straight for your exams and clinical rounds, I've put together a comparison table and a diagnostic flowchart.
| Feature | Appendicitis | Bowel Obstruction | Perforation |
|---|---|---|---|
| Pain Onset | Gradual (Periumbilical $\rightarrow$ RLQ) | Sudden, Colicky/Crampy | Sudden, "Explosive" |
| Vomiting | Follows pain | Early (High SBO) or Late (Low SBO) | Variable |
| Physical Exam | McBurney's tenderness, Guarding | Distension, Tinkling BS | Rigid, Board-like abdomen |
| Key Imaging | CT (Adults), US (Kids/Pregnancy) | X-ray (Air-fluid levels) | Upright CXR (Free air) |
| Initial Step | NPO, IV Fluids, Antibiotics | NPO, NG Tube decompression | NPO, IV Fluids, Emergent Surgery |
The comparison table and algorithm should give you a solid framework for these emergencies. Remember, the most important first step in any patient with a suspected perforation or high-grade obstruction is making them NPO (nothing by mouth) and starting aggressive IV fluid resuscitation.
For appendicitis, keep an eye out for the Alvarado Score (MANTRELS mnemonic) in your exams—it's a classic way to decide who needs imaging versus who goes straight to the OR.
Would you like to try some practice questions on these topics to see how they're tested, or should we look at some flashcards for the key physical exam signs?
Setting up chat...