
Scarring process and management — MCQs

A 30-year-old man comes to the physician for a follow-up examination 1 month after sustaining a chemical burn over the dorsum of his right hand and forearm. Physical examination shows hyperextension of the hand at the wrist. The skin over the dorsum of the wrist is tense and there is a thick, epithelialized scar. Range of motion of the right wrist is restricted. This patient's contracture is most likely due to activity of which of the following cells?
During examination of a stab wound, a forensic pathologist notes that one end is sharp and pointed while the other is square or blunt. The wound track shows a consistent width. Which of the following weapon characteristics is most likely?
A 35-year-old woman with no significant past medical, past surgical, family or social history presents to clinic with a recently identified area of flat, intact, pigmented skin. The patient believes that this is a large freckle, and she states that it becomes darker during the summer when she is outdoors. On physical examination, you measure the lesion to be 6 mm in diameter. Which of the following is the best descriptor of this patient’s skin finding?
A 48-year-old man is brought to the emergency department with a stab wound to his chest. The wound is treated in the emergency room. Three months later he develops a firm 4 x 3 cm nodular mass with intact epithelium over the site of the chest wound. On local examination, the scar is firm, non-tender, and there is no erythema. The mass is excised and microscopic examination reveals fibroblasts with plentiful collagen. Which of the following processes is most likely related to the series of events mentioned above?
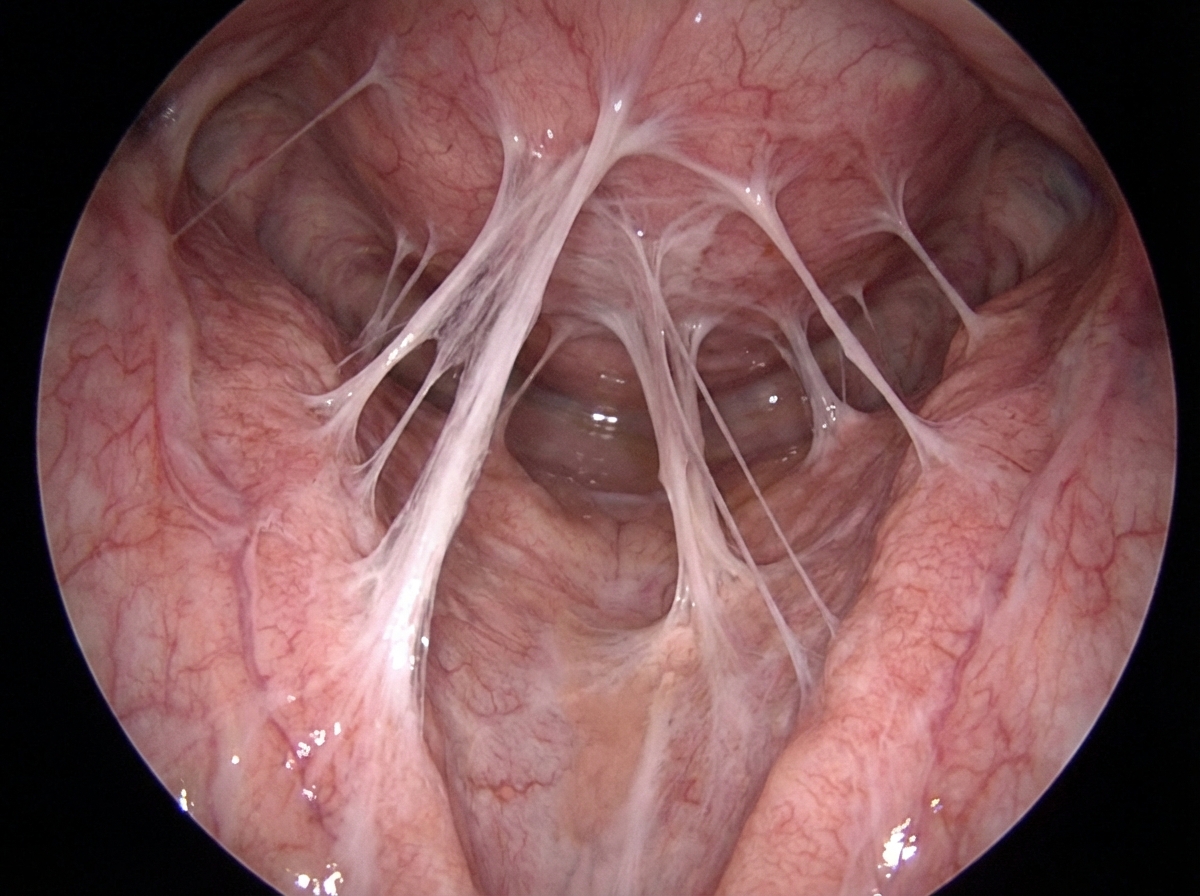
A 28-year-old woman and her husband are admitted to the office due to difficulties conceiving a child for the past year. Her menarche was at the age of 15 years, and her periods have been regular since then. Her medical history is positive for an abortion with curettage 5 years ago. A spermogram on the partner is performed, and it shows motile sperm cells. An ultrasound is performed on the patient and it is unremarkable. The laboratory results show that the FSH, LH, TSH, and prolactin levels are within normal ranges. A hysteroscopy is additionally performed and multiple adhesions are found in the uterus (refer to the image). Which of the following is the most likely composition of the scar tissue present in the uterus?
A 65-year-old woman presents to a dermatology clinic complaining about a couple of well-demarcated, dark, round skin lesions on her face. She claims she has had these lesions for 3 or 4 years. The lesions are painless, not pruritic, and have never bled. However, she is moderately distressed about the potential malignancy of these lesions after she heard that a close friend was just diagnosed with a melanoma. The medical history is unremarkable. Physical examination reveals a few well-demarcated, round, verrucous lesions, with a stuck-on appearance, distributed on the patient's back and face (see image). Under a dermatoscope, the lesions showed multiple comedo-like openings, milia cysts, and a cerebriform pattern. What is the best next step of management?

A 16-year-old boy presents to the emergency department after a skateboarding accident. He fell on a broken bottle and received a 4 cm wound on the dorsal aspect of his left hand. His vitals are stable and he was evaluated by the surgeon on call who determined that suturing was not required. After several weeks the wound has almost completely healed (see image). Which of the following is the correct description of this patient's wound before healing?

A 60-year-old male presents with fatigue, dyspnea on exertion, and lower extremity edema. Physical examination reveals an elevated jugular venous pressure and an S3 heart sound. Which of the following medications is most likely to improve this patient's symptoms?
A 30-year-old woman dies shortly after admission to the emergency department. The family requests an autopsy to determine cause of death. During the autopsy, multiple linear, parallel marks are noted across her wrists. Which of the following patterns suggests these are hesitation marks rather than defensive wounds?
A 45-year-old man comes to his primary care provider for a routine visit. The patient mentions that while he was cooking 5 days ago, he accidentally cut himself with a meat cleaver and lost the skin at the tip of his finger. After applying pressure and ice, the bleeding stopped and he did not seek treatment. The patient is otherwise healthy and does not take any daily medications. The patient’s temperature is 98.2°F (36.8°C), blood pressure is 114/72 mmHg, pulse is 60/min, and respirations are 12/min. On exam, the patient demonstrates a 0.5 x 0.3 cm wound on the tip of his left third finger. No bone is involved, and the wound is red, soft, and painless. There are no signs of infection. Which of the following can be expected on histopathological examination of the wounded area?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app