
Chronic wounds pathophysiology — MCQs

A researcher is studying the ability of breast cancer cells to metastasize. Neoplastic cells obtained from 30 patients with stage IV ductal carcinoma of the breast are tagged with a fluorescent antibody. The cells are then inserted into a medium resembling normal human tissue. After 2 weeks, all samples show in vitro hematogenous invasion and migration away from the original site of insertion. Which of the following properties is most likely responsible for the ability of these neoplastic cells to metastasize?
A 68-year-old woman comes to the physician because of a 3-month history of an oozing, red area above the left ankle. She does not recall any trauma to the lower extremity. She has type 2 diabetes mellitus, hypertension, atrial fibrillation, and ulcerative colitis. She had a myocardial infarction 2 years ago and a stroke 7 years ago. She has smoked 2 packs of cigarettes daily for 48 years and drinks 2 alcoholic beverages daily. Current medications include warfarin, metformin, aspirin, atorvastatin, carvedilol, and mesalamine. She is 165 cm (5 ft 4 in) tall and weighs 67 kg (148 lb); BMI is 24.6 kg/m2. Her temperature is 36.7°C (98°F), pulse is 90/min, respirations are 12/min, and blood pressure is 135/90 mm Hg. Examination shows yellow-brown spots and dilated tortuous veins over the lower extremities. The feet and the left calf are edematous. Femoral, popliteal, and pedal pulses are palpable bilaterally. There is a 3-cm (1.2-in) painless, shallow, exudative ulcer surrounded by granulation tissue above the medial left ankle. There is slight drooping of the right side of the face. Which of the following is the most likely cause of this patient's ulcer?
A 62-year-old man comes to the physician because of an oozing skin ulceration on his foot for 1 week. He has a history of type 2 diabetes mellitus and does not adhere to his medication regimen. Physical exam shows purulent discharge from an ulcer on the dorsum of his left foot. Pinprick sensation is decreased bilaterally to the level of the mid-tibia. A culture of the wound grows beta-hemolytic, coagulase-positive cocci in clusters. The causal organism most likely produces which of the following virulence factors?
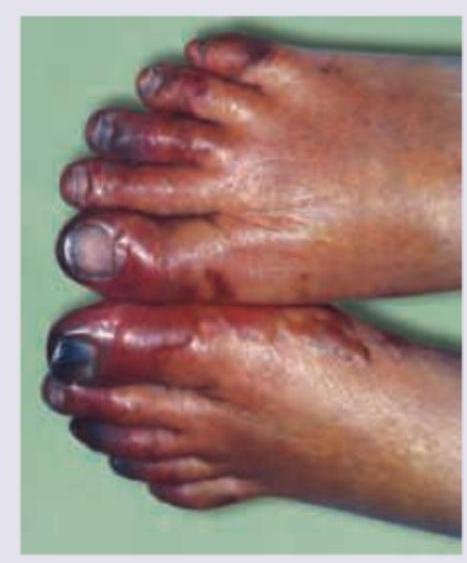
A 42-year-old man presents to the clinic for a second evaluation of worsening blackened ulcers on the tips of his toes. His past medical history includes diabetes mellitus for which he takes metformin and his most recent HbA1c was 6.0, done 3 months ago. He also has hypertension for which he's prescribed amlodipine and chronic obstructive pulmonary disease (COPD) for which he uses an albuterol-ipratropium combination inhaler. He is also a chronic tobacco user with a 27-pack-year smoking history. He first noticed symptoms of a deep aching pain in his toes. Several months ago, he occasionally felt pain in his fingertips both at rest and with activity. Now he reports blackened skin at the tips of his fingers and toes. Evaluation shows: pulse of 82/min, blood pressure of 138/85 mm Hg, oral temperature 37.0°C (98.6°F). He is thin. Physical examination of his feet demonstrates the presence of 3, 0.5–0.8 cm, eschars over the tips of his bilateral second toes and right third toe. There is no surrounding erythema or exudate. Proprioception, vibratory sense, and monofilament examination are normal on both ventral aspects of his feet, but he lacks sensation over the eschars. Dorsal pedal pulses are diminished in both feet; the skin is shiny and hairless. Initial lab results include a C-reactive protein (CRP) level of 3.5 mg/dL, leukocytes of 6,000/mm3, erythrocyte sedimentation rate (ESR) of 34 mm/hr, and negative antinuclear antibodies. Which part of the patient's history is most directly associated with his current problem?
A 31-year-old woman scrapes her finger on an exposed nail and sustains a minor laceration. Five minutes later, her finger is red, swollen, and painful. She has no past medical history and does not take any medications. She drinks socially with her friends and does not smoke. The inflammatory cell type most likely to be prominent in this patient's finger has which of the following characteristics?
A 72-year-old man comes to the emergency department because of severe, acute, right leg pain for 2 hours. The patient's symptoms started suddenly while he was doing household chores. He has no history of leg pain at rest or with exertion. Yesterday, he returned home after a 6-hour bus ride from his grandson's home. He has hypertension treated with ramipril. He appears uncomfortable. His temperature is 37.4°C (99.3°F), pulse is 105/min and irregular, and blood pressure is 146/92 mm Hg. The right lower extremity is cool and tender to touch. A photograph of the limb is shown. Femoral pulses are palpable bilaterally; popliteal and pedal pulses are decreased on the right side. Sensation to pinprick and light touch and muscle strength are decreased in the right lower extremity. Which of the following is most likely to confirm the underlying source of this patient's condition?
A 45-year-old man comes to his primary care provider for a routine visit. The patient mentions that while he was cooking 5 days ago, he accidentally cut himself with a meat cleaver and lost the skin at the tip of his finger. After applying pressure and ice, the bleeding stopped and he did not seek treatment. The patient is otherwise healthy and does not take any daily medications. The patient’s temperature is 98.2°F (36.8°C), blood pressure is 114/72 mmHg, pulse is 60/min, and respirations are 12/min. On exam, the patient demonstrates a 0.5 x 0.3 cm wound on the tip of his left third finger. No bone is involved, and the wound is red, soft, and painless. There are no signs of infection. Which of the following can be expected on histopathological examination of the wounded area?
A 63-year-old man presents to the clinic complaining of burning bilateral leg pain which has been increasing gradually over the past several months. It worsens when he walks but improves with rest. His past medical and surgical history are significant for hypertension, hyperlipidemia, diabetes, and a 40-pack-year smoking history. His temperature is 99.0°F (37.2°C), blood pressure is 167/108 mm Hg, pulse is 88/min, respirations are 13/min, and oxygen saturation is 95% on room air. Physical exam of the lower extremities reveals palpable but weak posterior tibial and dorsalis pedis pulses bilaterally. Which of the following is the best initial treatment for this patient's symptoms?
A 54-year-old man comes to the physician because of a painful mass in his left thigh for 3 days. He underwent a left lower limb angiography for femoral artery stenosis and had a stent placed 2 weeks ago. He has peripheral artery disease, coronary artery disease, hypercholesterolemia and type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for 34 years. Current medications include enalapril, aspirin, simvastatin, metformin, and sitagliptin. His temperature is 36.7°C (98°F), pulse is 88/min, and blood pressure is 116/72 mm Hg. Examination shows a 3-cm (1.2-in) tender, pulsatile mass in the left groin. The skin over the area of the mass shows no erythema and is cool to the touch. A loud bruit is heard on auscultation over this area. The remainder of the examination shows no abnormalities. Results of a complete blood count and serum electrolyte concentrations show no abnormalities. Duplex ultrasonography shows an echolucent sac connected to the common femoral artery, with pulsatile and turbulent blood flow between the artery and the sac. Which of the following is the most appropriate next best step in management?
A 65-year-old man comes to the emergency department because of sudden, worsening pain in his right calf and foot that started 30 minutes ago. He also has a tingling sensation and weakness in his right leg. He has had no similar episodes, recent trauma, or claudication. He has type 2 diabetes mellitus and was diagnosed with hypertension 20 years ago. His sister has systemic sclerosis. He works as an office administrator and sits at his desk most of the day. He has smoked one and a half packs of cigarettes daily for 30 years. Current medications include metformin and lisinopril. His pulse is 110/min, respirations are 16/min, and blood pressure is 140/90 mm Hg. His right leg is pale and cool to touch. Muscle strength in his right leg is mildly reduced. Pedal pulses are absent on the right. Which of the following is the most likely underlying cause of this patient's symptoms?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app