
Wound healing — MCQs

On this page
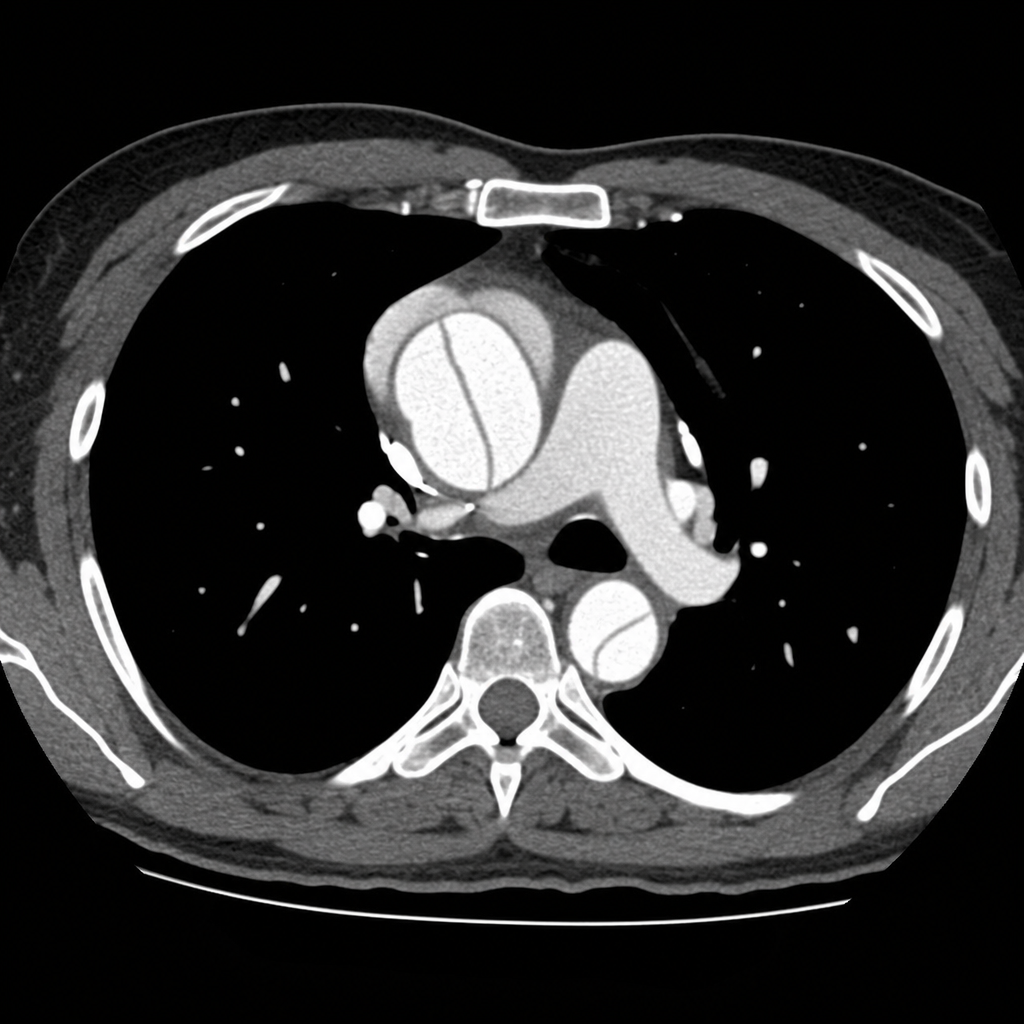
A 45-year-old woman presents to the emergency department with sudden-onset tearing chest pain radiating to her back. She has a history of hypertension and is a current smoker. Blood pressure is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. Heart rate is 96 bpm. She is diaphoretic but alert and oriented. Chest radiograph shows a widened mediastinum. CT chest with IV contrast demonstrates a Stanford Type A aortic dissection with an intimal flap involving the ascending aorta. After initiating IV beta-blockade for immediate heart rate and blood pressure control, which of the following is the most appropriate next step in definitive management?
A 42-year-old man sustains a deep laceration requiring surgical debridement. The wound care team debates between primary closure versus healing by secondary intention. The wound is 6 cm long, 2 cm wide, located on the lower leg with mild contamination from soil exposure, and the patient is a heavy smoker with peripheral vascular disease. Evaluate which approach best synthesizes the risk-benefit analysis for optimal outcome?
A 35-year-old woman with known deficiency in Ehlers-Danlos syndrome presents with recurrent wound dehiscence following multiple abdominal surgeries. Genetic testing confirms a mutation affecting type III collagen synthesis. She now requires another laparotomy for adhesive bowel obstruction. The surgical team must decide on closure technique. Synthesizing knowledge of collagen biochemistry and surgical principles, which approach best addresses her specific wound healing defect?
A 58-year-old man with chronic kidney disease (creatinine 4.2 mg/dL) and uremia undergoes arteriovenous fistula creation for dialysis access. Four weeks postoperatively, the wound continues to show poor healing with minimal tensile strength. Laboratory studies show elevated blood urea nitrogen. Considering the multiple factors affecting wound healing in uremia, evaluate which intervention would most comprehensively address the wound healing deficit?
A 50-year-old woman undergoes wide local excision of a melanoma from her back. The pathologist reports that the wound healing specimen shows granulation tissue with parallel capillary loops perpendicular to the wound surface, active fibroblast proliferation, and myofibroblast presence causing wound contraction. Analysis of these findings indicates the wound is in which phase, and what is the primary cellular source of the contractile forces?
Practice by Chapter
Phases of wound healing
Practice Questions
Primary vs. secondary intention
Practice Questions
Types of wound closure
Practice Questions
Factors affecting wound healing
Practice Questions
Chronic wounds pathophysiology
Practice Questions
Diabetic wounds
Practice Questions
Pressure ulcers staging and management
Practice Questions
Surgical wound classification
Practice Questions
Wound assessment techniques
Practice Questions
Advanced wound care products
Practice Questions
Negative pressure wound therapy
Practice Questions
Hyperbaric oxygen therapy
Practice Questions
Scarring process and management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app