
Thoracic aortic aneurysm management — MCQs

A 72-year-old woman comes to the physician for follow-up care. One year ago, she was diagnosed with a 3.8-cm infrarenal aortic aneurysm found incidentally on abdominal ultrasound. She has no complaints. She has hypertension, type 2 diabetes mellitus, and COPD. Current medications include hydrochlorothiazide, lisinopril, glyburide, and an albuterol inhaler. She has smoked a pack of cigarettes daily for 45 years. Her temperature is 37°C (98.6°F), pulse is 90/min, respirations are 12/min, and blood pressure is 145/85 mm Hg. Examination shows a faint abdominal bruit on auscultation. Ultrasonography of the abdomen shows a 4.9-cm saccular dilation of the infrarenal aorta. Which of the following is the most appropriate next step in management?
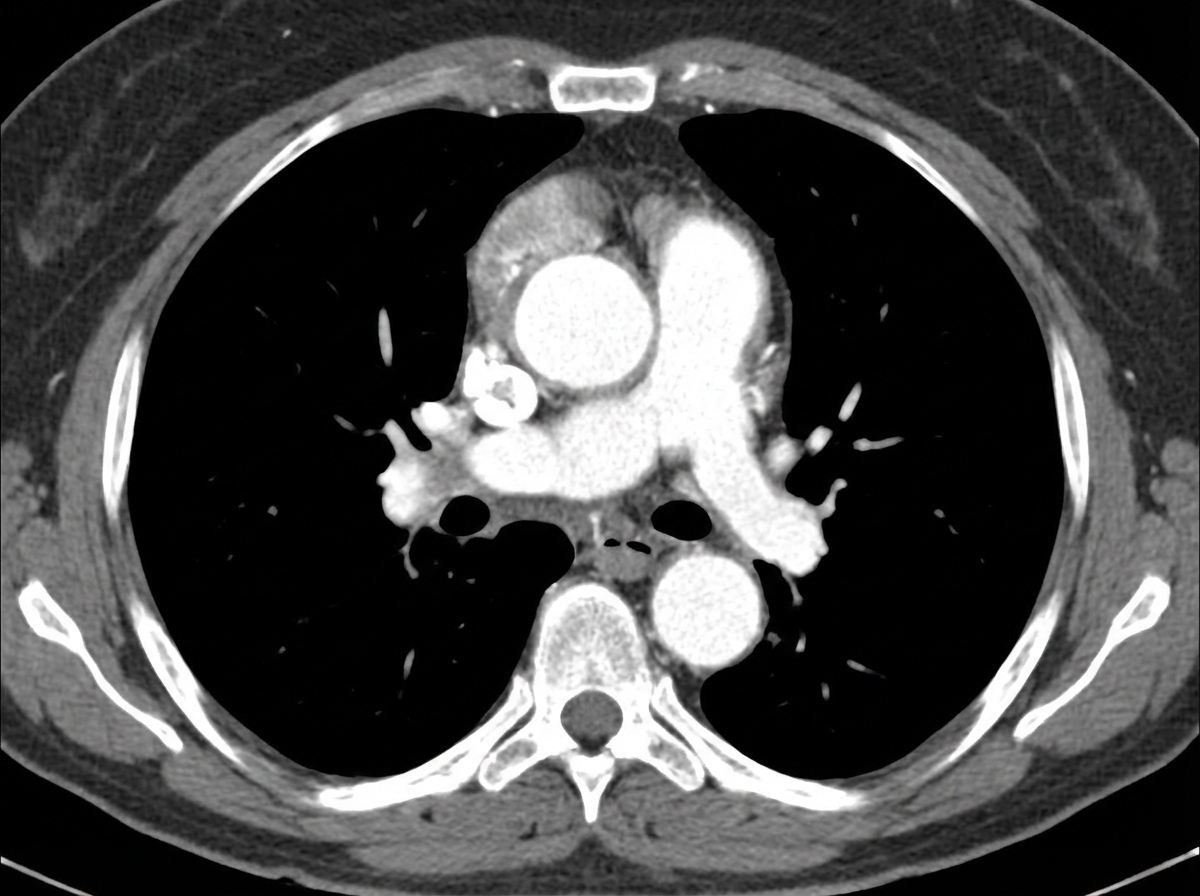
A 43-year-old man from Chile comes to the physician because of a 1-day history of upper back pain and difficulty swallowing. He has had pain in his shoulder and knee joints over the past 10 years. He is 190 cm (6 ft 3 in) tall and weighs 70.3 kg (155 lb); BMI is 19.4 kg/m2. His blood pressure is 142/86 mm Hg in the right arm and 130/70 mm Hg in the left arm. Physical examination shows a depression in the sternum and a grade 3/6 diastolic murmur at the right upper sternal border. A CT scan of the chest with contrast is shown. Which of the following is the most likely underlying cause of this patient's condition?
A 58-year-old man is brought to the emergency department by his family because of severe upper back pain, which he describes as ripping. The pain started suddenly 1 hour ago while he was watching television. He has hypertension for 13 years, but he is not compliant with his medications. He denies the use of nicotine, alcohol or illicit drugs. His temperature is 36.5°C (97.7°F), the heart rate is 110/min and the blood pressure is 182/81 mm Hg in the right arm and 155/71 mm Hg in the left arm. CT scan of the chest shows an intimal flap limited to the descending aorta. Intravenous opioid analgesia is started. Which of the following is the best next step in the management of this patient condition?
A 68-year-old man presents for a screening ultrasound scan. He has been feeling well and is in his usual state of good health. His medical history is notable for mild hypertension and a 100-pack-year tobacco history. He has a blood pressure of 128/86 and heart rate of 62/min. Physical examination is clear lung sounds and regular heart sounds. On ultrasound, an infrarenal aortic aneurysm of 4 cm in diameter is identified. Which of the following is the best initial step for this patient?
A 55-year-old man is brought to the emergency department 30 minutes after the sudden onset of severe, migrating anterior chest pain, shortness of breath, and sweating at rest. He has hypertension, hypercholesterolemia, and type 2 diabetes mellitus. Medications include atorvastatin, hydrochlorothiazide, lisinopril, and metformin. He has smoked one pack of cigarettes daily for 25 years. He is in severe distress. His pulse is 110/min, respirations are 20/min, and blood pressure is 150/85 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. Cardiac examination shows a grade 3/6, high-pitched, blowing, diastolic murmur heard best over the right sternal border. The lungs are clear to auscultation. Femoral pulses are decreased bilaterally. An ECG shows sinus tachycardia and left ventricular hypertrophy. Which of the following is the most likely diagnosis?
A 10-month-old boy is brought to the clinic with a history of recurrent episodes of stridor and wheezing. His mother reports that his wheezing is exacerbated by crying, feeding, and flexion of the neck, and is relieved by extension of the neck. Occasionally he vomits after feeding. What is the most likely diagnosis?
A 43-year-old man comes to the physician because of increasing shortness of breath for 1 month. He has been using two pillows at night but frequently wakes up feeling as if he is choking. Five months ago, he underwent surgery for creation of an arteriovenous fistula in his left upper arm. He has hypertension and chronic kidney disease due to reflux nephropathy. He receives hemodialysis three times a week. His current medications are enalapril, vitamin D3, erythropoietin, sevelamer, and atorvastatin. His temperature is 37.1°C (98.8°F), respirations are 22/min, pulse is 103/min and bounding, and blood pressure is 106/58 mm Hg. Examination of the lower extremities shows bilateral pitting pedal edema. There is jugular venous distention. A prominent thrill is heard over the brachiocephalic arteriovenous fistula. There are crackles heard at both lung bases. Cardiac examination shows an S3 gallop. The abdomen is soft and nontender. Which of the following is the most likely cause of this patient's symptoms?
A 75-year-old Caucasian man presents to the emergency department with abdominal pain. The patient states he was at home eating dinner when he began to experience severe abdominal pain. The patient has a past medical history of diabetes, hypertension, and atherosclerosis. He lives at home alone, smokes cigarettes, and drinks 1 to 2 alcoholic drinks per day. The patient is given IV morphine and an ultrasound is obtained demonstrating a dilated abdominal aorta. The patient states that his father died of a similar finding and is concerned about his prognosis. Which of the following is the greatest risk factor for this patient's presentation?
In a routine medical examination, a young man is noted to be tall with slight scoliosis and pectus excavatum. He had been told that he was over the 95% percentile for height as a child. Auscultation reveals a heart murmur, and transthoracic echocardiography shows an enlarged aortic root and mitral valve prolapse. Blood screening for fibrillin-1 (FBN1) gene mutation is positive and plasma homocysteine is normal. This patient is at high risk for which of the following complications?
A 67-year-old man presents to the emergency department with abdominal pain that started 1 hour ago. The patient has a past medical history of diabetes and hypertension as well as a 40 pack-year smoking history. His blood pressure is 107/58 mmHg, pulse is 130/min, respirations are 23/min, and oxygen saturation is 98% on room air. An abdominal ultrasound demonstrates focal dilation of the aorta with peri-aortic fluid. Which of the following is the best next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app