
Endovascular procedures overview — MCQs

A 72-year-old woman comes to the physician for follow-up care. One year ago, she was diagnosed with a 3.8-cm infrarenal aortic aneurysm found incidentally on abdominal ultrasound. She has no complaints. She has hypertension, type 2 diabetes mellitus, and COPD. Current medications include hydrochlorothiazide, lisinopril, glyburide, and an albuterol inhaler. She has smoked a pack of cigarettes daily for 45 years. Her temperature is 37°C (98.6°F), pulse is 90/min, respirations are 12/min, and blood pressure is 145/85 mm Hg. Examination shows a faint abdominal bruit on auscultation. Ultrasonography of the abdomen shows a 4.9-cm saccular dilation of the infrarenal aorta. Which of the following is the most appropriate next step in management?
A 16-year-old boy comes to the physician for a routine health maintenance examination. He feels well. He has no history of serious illness. He is at the 60th percentile for height and weight. Vital signs are within normal limits. The lungs are clear to auscultation. A grade 3/6 ejection systolic murmur is heard along the lower left sternal border. The murmur decreases in intensity on rapid squatting and increases in intensity when he performs the Valsalva maneuver. This patient is at increased risk for which of the following complications?
A 27-year-old soldier stationed in Libya sustains a shrapnel injury during an attack, causing a traumatic above-elbow amputation. The resulting arterial bleed is managed with a tourniquet prior to transport to the military treatment facility. On arrival, he is alert and oriented to person, place, and time. His armor and clothing are removed. His pulse is 145/min, respirations are 28/min, and blood pressure is 95/52 mm Hg. Pulmonary examination shows symmetric chest rise. The lungs are clear to auscultation. Abdominal examination shows no abnormalities. There are multiple shrapnel wounds over the upper and lower extremities. A tourniquet is in place around the right upper extremity; the right proximal forearm has been amputated. One large-bore intravenous catheter is placed in the left antecubital fossa. Despite multiple attempts, medical staff is unable to establish additional intravenous access. Which of the following is the most appropriate next step in management?
One and a half hours after undergoing an elective cardiac catheterization, a 53-year-old woman has right flank and back pain. She has hypertension, hypercholesterolemia, and type 2 diabetes mellitus. She had an 80% stenosis in the left anterior descending artery and 2 stents were placed. Intravenous unfractionated heparin was used prior to the procedure. Prior to admission, her medications were enalapril, simvastatin, and metformin. Her temperature is 37.3°C (99.1°F), pulse is 102/min, and blood pressure is 109/75 mm Hg. Examination shows a tender lower abdomen; there is no guarding or rigidity. There is right suprainguinal fullness and tenderness. There is no bleeding or discharge from the femoral access site. Cardiac examination shows no murmurs, rubs, or gallops. Femoral and pedal pulses are palpable bilaterally. 0.9% saline infusion is begun. A complete blood count shows a hematocrit of 36%, leukocyte count of 8,400/mm3, and a platelet count of 230,000/mm3. Which of the following is the most appropriate next step in management?
A 17-year-old teenager is brought to the emergency department with severe bleeding from his right hand. He was involved in a gang fight about 30 minutes ago where he received a penetrating stab wound by a sharp knife in the region of the ‘anatomical snuffbox’. A vascular surgeon is called in for consultation. Damage to which artery is most likely responsible for his excessive bleeding?
A 55-year-old man comes to the emergency department because of left-sided chest pain and difficulty breathing for the past 30 minutes. His pulse is 88/min. He is pale and anxious. Serum studies show increased cardiac enzymes. An ECG shows ST-elevations in leads I, aVL, and V5-V6. A percutaneous coronary intervention is performed. In order to localize the site of the lesion, the catheter must pass through which of the following structures?
A 33-year-old woman comes to the emergency department because of severe right flank pain for 2 hours. The pain is colicky in nature and she describes it as 9 out of 10 in intensity. She has had 2 episodes of vomiting. She has no history of similar episodes in the past. She is 160 cm (5 ft 3 in) tall and weighs 104 kg (229 lb); BMI is 41 kg/m2. Her temperature is 37.3°C (99.1°F), pulse is 96/min, respirations are 16/min and blood pressure is 116/76 mm Hg. The abdomen is soft and there is mild tenderness to palpation in the right lower quadrant. Bowel sounds are reduced. The remainder of the examination shows no abnormalities. Her leukocyte count is 7,400/mm3. A low-dose CT scan of the abdomen and pelvis shows a round 12-mm stone in the distal right ureter. Urine dipstick is mildly positive for blood. Microscopic examination of the urine shows RBCs and no WBCs. 0.9% saline infusion is begun and intravenous ketorolac is administered. Which of the following is the most appropriate next step in management?
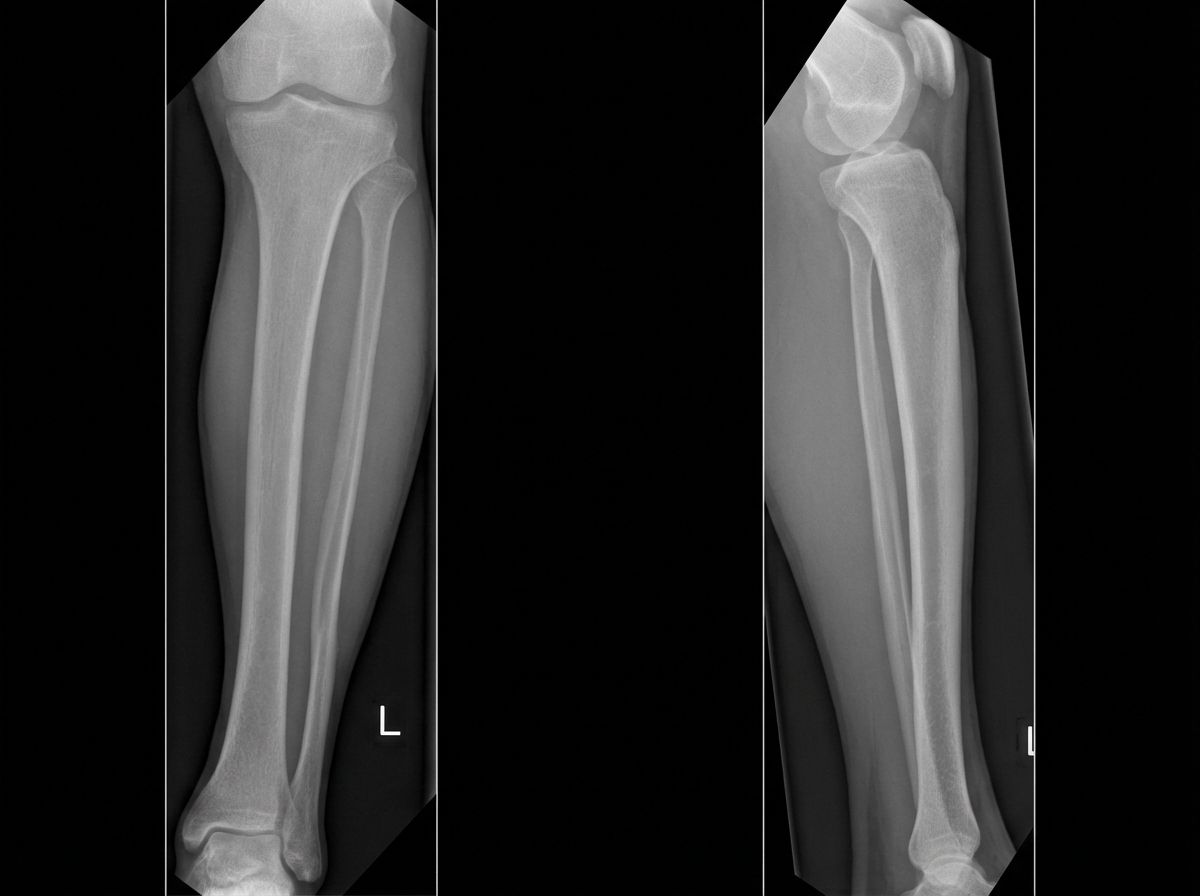
A 36-year-old man comes to the emergency department 4 hours after a bike accident for severe pain and swelling in his right leg. He has not had a headache, nausea, vomiting, abdominal pain, or blood in his urine. He has a history of gastroesophageal reflux disease and allergic rhinitis. He has smoked one pack of cigarettes daily for 17 years and drinks an average of one alcoholic beverage daily. His medications include levocetirizine and pantoprazole. He is in moderate distress. His temperature is 37°C (98.6°F), pulse is 112/min, and blood pressure is 140/80 mm Hg. Examination shows multiple bruises over both lower extremities and the face. There is swelling surrounding a 2 cm laceration 13 cm below the right knee. The lower two-thirds of the tibia is tender to palpation and the skin is pale and cool to the touch. The anterior tibial, posterior tibial, and dorsalis pedis pulses are weak. Capillary refill time of the right big toe is 4 seconds. Dorsiflexion of his right foot causes severe pain in his calf. Cardiopulmonary examination is normal. An x-ray is ordered, which is shown below. Which of the following is the most appropriate next step in management?
A 59-year-old patient comes to the emergency department accompanied by his wife because of severe right leg pain and numbness. His condition suddenly started an hour ago. His wife says that he has a heart rhythm problem for which he takes a blood thinner, but he is not compliant with his medications. He has smoked 10–15 cigarettes daily for the past 15 years. His temperature is 36.9°C (98.42°F), blood pressure is 140/90 mm Hg, and pulse is 85/min and irregular. On physical examination, the patient is anxious and his right leg is cool and pale. Palpation of the popliteal fossa shows a weaker popliteal pulse on the right side compared to the left side. Which of the following is the best initial step in the management of this patient's condition?
A 62-year-old man presents to the emergency department with sudden onset of severe left leg pain accompanied by numbness and weakness. His medical history is remarkable for hypertension and hyperlipidemia. His vital signs include a blood pressure of 155/92 mm Hg, a temperature of 37.1°C (98.7°F), and an irregular pulse of 92/min. Physical examination reveals absent left popliteal and posterior tibial pulses. His left leg is noticeably cold and pale. There is no significant tissue compromise, nerve damage, or sensory loss. Which of the following will most likely be required for this patient's condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app