
Acute limb ischemia management — MCQs

A 65-year-old man is referred by his primary care provider to a neurologist for leg pain. He reports a 6-month history of progressive bilateral lower extremity pain that is worse in his left leg. The pain is 5/10 in severity at its worst and is described as a "burning" pain. He has noticed that the pain is acutely worse when he walks downhill. He has started riding his stationary bike more often as it relieves his pain. His past medical history is notable for hypertension, diabetes mellitus, and a prior myocardial infarction. He also sustained a distal radius fracture the previous year after falling on his outstretched hand. He takes aspirin, atorvastatin, metformin, glyburide, enalapril, and metoprolol. He has a 30-pack-year smoking history and drinks 2-3 glasses of wine with dinner every night. His temperature is 99°F (37.2°C), blood pressure is 145/85 mmHg, pulse is 91/min, and respirations are 18/min. On exam, he is well-appearing and in no acute distress. A straight leg raise is negative. A valsalva maneuver does not worsen his pain. Which of the following is the most appropriate test to confirm this patient's diagnosis?
A 20-year-old woman is brought to the emergency department because of severe muscle soreness, nausea, and darkened urine for 2 days. The patient is on the college track team and has been training intensively for an upcoming event. One month ago, she had a urinary tract infection and was treated with nitrofurantoin. She appears healthy. Her temperature is 37°C (98.6°F), pulse is 64/min, and blood pressure is 110/70 mm Hg. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and non-tender. There is diffuse muscle tenderness over the arms, legs, and back. Laboratory studies show: Hemoglobin 12.8 g/dL Leukocyte count 7,000/mm3 Platelet count 265,000/mm3 Serum Creatine kinase 22,000 U/L Lactate dehydrogenase 380 U/L Urine Blood 3+ Protein 1+ RBC negative WBC 1–2/hpf This patient is at increased risk for which of the following complications?
A 54-year-old man comes to the emergency department because of severe pain in his right leg that began suddenly 3 hours ago. He has had repeated cramping in his right calf while walking for the past 4 months, but it has never been this severe. He has type 2 diabetes mellitus, hypercholesterolemia, and hypertension. Current medications include insulin, enalapril, aspirin, and simvastatin. He has smoked one pack of cigarettes daily for 33 years. He does not drink alcohol. His pulse is 103/min and blood pressure is 136/84 mm Hg. Femoral pulses are palpable bilaterally. The popliteal and pedal pulses are absent on the right. Laboratory studies show: Hemoglobin 16.1 g/dL Serum Urea nitrogen 14 mg/dL Glucose 166 mg/dL Creatinine 1.5 mg/dL A CT angiogram of the right lower extremity is ordered. Which of the following is the most appropriate next step in management?
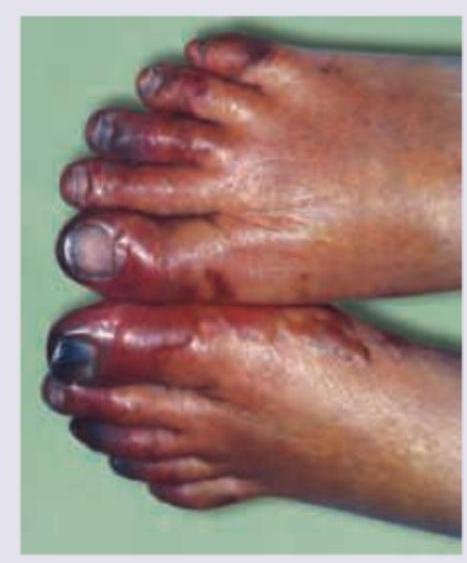
Two days after undergoing emergency cardiac catherization for myocardial infarction, a 68-year-old woman has pain in her toes. During the intervention, she was found to have an occluded left anterior descending artery and 3 stents were placed. She has hypertension, hypercholesterolemia, and coronary artery disease. Prior to admission, her medications were metoprolol, enalapril, atorvastatin, and aspirin. Her temperature is 37.3°C (99.1°F), pulse is 93/min, and blood pressure is 115/78 mm Hg. Examination shows discoloration of the toes of both feet. A photograph of the right foot is shown. The lesions are cool and tender to palpation. The rest of the skin on the feet is warm; femoral and pedal pulses are palpable bilaterally. This patient is at increased risk for which of the following conditions?

A 68-year-old man presents to the emergency department with leg pain. He states that the pain started suddenly while he was walking outside. The patient has a past medical history of diabetes, hypertension, obesity, and atrial fibrillation. His temperature is 99.3°F (37.4°C), blood pressure is 152/98 mmHg, pulse is 97/min, respirations are 15/min, and oxygen saturation is 99% on room air. Physical exam is notable for a cold and pale left leg. The patient’s sensation is markedly diminished in the left leg when compared to the right, and his muscle strength is 1/5 in his left leg. Which of the following is the best next step in management?
A 72-year-old man comes to the emergency department because of severe, acute, right leg pain for 2 hours. The patient's symptoms started suddenly while he was doing household chores. He has no history of leg pain at rest or with exertion. Yesterday, he returned home after a 6-hour bus ride from his grandson's home. He has hypertension treated with ramipril. He appears uncomfortable. His temperature is 37.4°C (99.3°F), pulse is 105/min and irregular, and blood pressure is 146/92 mm Hg. The right lower extremity is cool and tender to touch. A photograph of the limb is shown. Femoral pulses are palpable bilaterally; popliteal and pedal pulses are decreased on the right side. Sensation to pinprick and light touch and muscle strength are decreased in the right lower extremity. Which of the following is most likely to confirm the underlying source of this patient's condition?
A 75-year-old man presents to the emergency department because of pain in his left thigh and left calf for the past 3 months. The pain occurs at rest, increases with walking, and is mildly improved by hanging the foot off the bed. He has had hypertension for 25 years and type 2 diabetes mellitus for 30 years. He has smoked 30–40 cigarettes per day for the past 45 years. On examination, femoral, popliteal, and dorsalis pedis pulses are faint on both sides. The patient’s foot is shown in the image. Resting ankle-brachial index (ABI) is found to be 0.30. Antiplatelet therapy and aggressive risk factors modifications are initiated. Which of the following is the best next step for this patient?
A 25-year-old patient is brought into the emergency department after he was found down by the police in 5 degree celsius weather. The police state the patient is a heroin-user and is homeless. The patient's vitals are T 95.3 HR 80 and regular BP 150/90 RR 10. After warming the patient, you notice his left lower leg is now much larger than his right leg. On exam, the patient has a loss of sensation on his left lower extremity. There is a faint palpable dorsalis pedal pulse, but no posterior tibial pulse. The patient is unresponsive to normal commands, but shrieks in pain upon passive stretch of his left lower leg. What is the most probable cause of this patient's condition?
Four days after undergoing a craniotomy and evacuation of a subdural hematoma, a 56-year-old man has severe pain and swelling of his right leg. He has chills and nausea. He has type 2 diabetes mellitus and chronic kidney disease, and was started on hemodialysis 2 years ago. Prior to admission, his medications were insulin, enalapril, atorvastatin, and sevelamer. His temperature is 38.3°C (101°F), pulse is 110/min, and blood pressure is 130/80 mm Hg. Examination shows a swollen, warm, and erythematous right calf. Dorsiflexion of the right foot causes severe pain in the right calf. The peripheral pulses are palpated bilaterally. Cardiopulmonary examination shows no abnormalities. Laboratory studies show: Hemoglobin 10.1 g/dL Leukocyte count 11,800/mm3 Platelet count 230,000/mm3 Serum Glucose 87 mg/dL Creatinine 1.9 mg/dL Which of the following is the most appropriate next step in treatment?
A 31-year-old man presents to the Emergency Department with severe left leg pain and paresthesias 4 hours after his leg got trapped by the closing door of a bus. Initially, he had a mild pain which gradually increased to unbearable levels. Past medical history is noncontributory. In the Emergency Department, his blood pressure is 130/80 mm Hg, heart rate is 87/min, respiratory rate is 14/min, and temperature is 36.8℃ (98.2℉). On physical exam, his left calf is firm and severely tender on palpation. The patient cannot actively dorsiflex his left foot, and passive dorsiflexion is limited. Posterior tibial and dorsalis pedis pulses are 2+ in the right leg and 1+ in the left leg. Axial load does not increase the pain. Which of the following is the best next step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app