
Vascular Surgery — MCQs

On this page
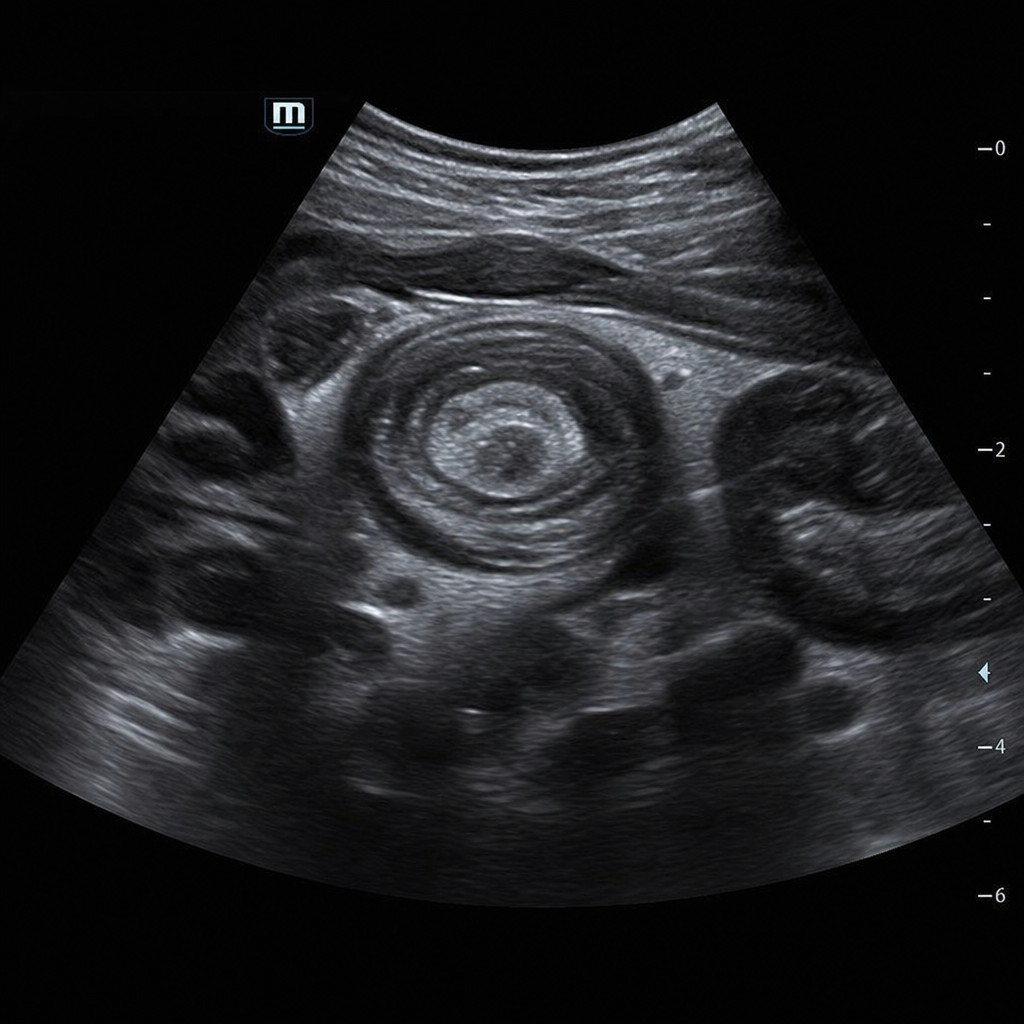
A 3-year-old boy is brought to the emergency department by his parents with a 12-hour history of intermittent, severe crampy abdominal pain that occurs in episodes lasting 2–3 minutes followed by periods during which the child appears completely well. He has had two episodes of vomiting and passed one stool described as 'red currant jelly.' On examination, his abdomen is soft between episodes with a sausage-shaped mass palpable in the right upper quadrant. An abdominal ultrasound is obtained and shows a target sign (concentric rings) in the right upper quadrant consistent with ileocolic intussusception. Which of the following is the most appropriate next step in management?
Practice by Chapter
Abdominal aortic aneurysm repair
Practice Questions
Acute limb ischemia management
Practice Questions
Aortic dissection management
Practice Questions
Bypass grafting techniques and materials
Practice Questions
Carotid endarterectomy indications and technique
Practice Questions
Compartment syndrome diagnosis and fasciotomy
Practice Questions
Dialysis access procedures and complications
Practice Questions
Endovascular procedures overview
Practice Questions
Peripheral arterial disease diagnosis and management
Practice Questions
Thoracic aortic aneurysm management
Practice Questions
Thromboembolectomy procedures
Practice Questions
Vascular trauma management
Practice Questions
Venous insufficiency and varicose vein treatment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app