
Trauma/Emergencies — MCQs

On this page
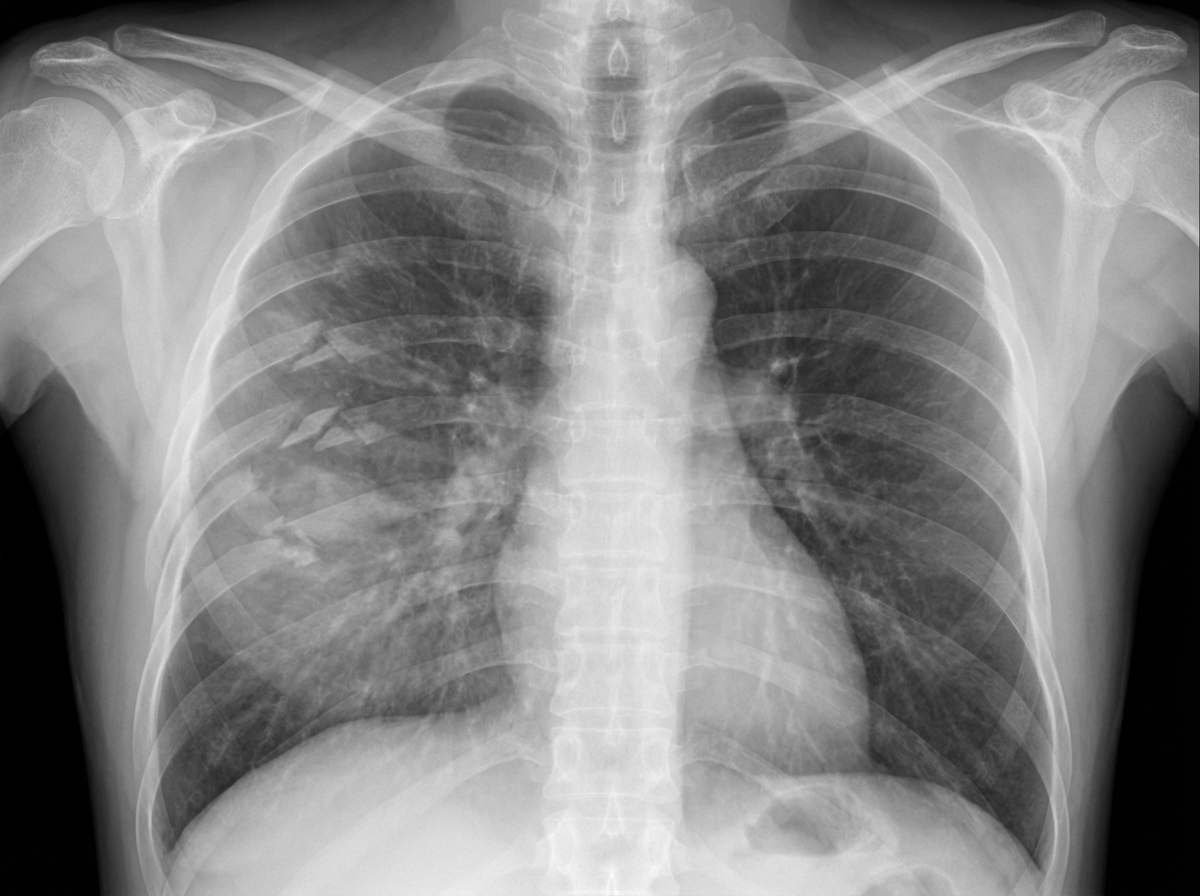
A 45-year-old man in respiratory distress presents to the emergency department. He sustained a stab to his left chest and was escorted to the nearest hospital. The patient appears pale and has moderate difficulty with breathing. His O2 saturation is 94%. The left lung is dull to percussion. CXRs are ordered and confirm the likely diagnosis. His blood pressure is 95/57 mm Hg, the respirations are 22/min, the pulse is 87/min, and the temperature is 36.7°C (98.0°F). His chest X-ray is shown. Which of the following is the next best step in management for this patient?

A 22-year-old man presents to the emergency department after being tackled in a game of football. The patient was hit from behind and fell to the ground. After the event, he complained of severe pain in his knee. The patient has a past medical history of anabolic steroid use. His current medications include whey protein supplements, multivitamins, and fish oil. His temperature is 99.5°F (37.5°C), blood pressure is 137/68 mmHg, pulse is 100/min, respirations are 17/min, and oxygen saturation is 98% on room air. On physical exam, you see a muscular young man clutching his knee in pain. The knee is inflamed and erythematous. When valgus stress is applied to the leg, there is some laxity when compared to the contralateral leg. The patient is requesting surgery for his injury. Arthrocentesis is performed and demonstrates no abnormalities of the synovial fluid. Which of the following physical exam findings is most likely to be seen in this patient?
A 40-year-old sailor is brought to a military treatment facility 20 minutes after being involved in a navy ship collision. He appears ill. He reports a sensation that he needs to urinate but is unable to void. His pulse is 140/min, respirations are 28/min, and blood pressure is 104/70 mm Hg. Pelvic examination shows ecchymoses over the scrotum and perineum. There is tenderness over the suprapubic region and blood at the urethral meatus. Digital rectal examination shows a high-riding prostate. Abdominal ultrasound shows a moderately distended bladder. X-rays of the pelvis show fractures of all four pubic rami. Which of the following is the most likely cause of this patient's symptoms?
A 62-year-old man is brought to the emergency department after his wife found him unresponsive 1 hour ago. He had fallen from a flight of stairs the previous evening. Four years ago, he underwent a mitral valve replacement. He has hypertension and coronary artery disease. Current medications include aspirin, warfarin, enalapril, metoprolol, and atorvastatin. On arrival, he is unconscious. His temperature is 37.3°C (99.1°F), pulse is 59/min, respirations are 7/min and irregular, and blood pressure is 200/102 mm Hg. The right pupil is 5 mm and fixed. The left pupil is 4 mm and reactive to light. There is extension of the extremities to painful stimuli. The lungs are clear to auscultation. Cardiac examination shows a systolic click. The abdomen is soft and nontender. He is intubated and mechanically ventilated. A mannitol infusion is begun. A noncontrast CT scan of the brain shows a 6-cm subdural hematoma on the right side with an 18-mm midline shift. Which of the following is the most likely early sequela of this patient's current condition?
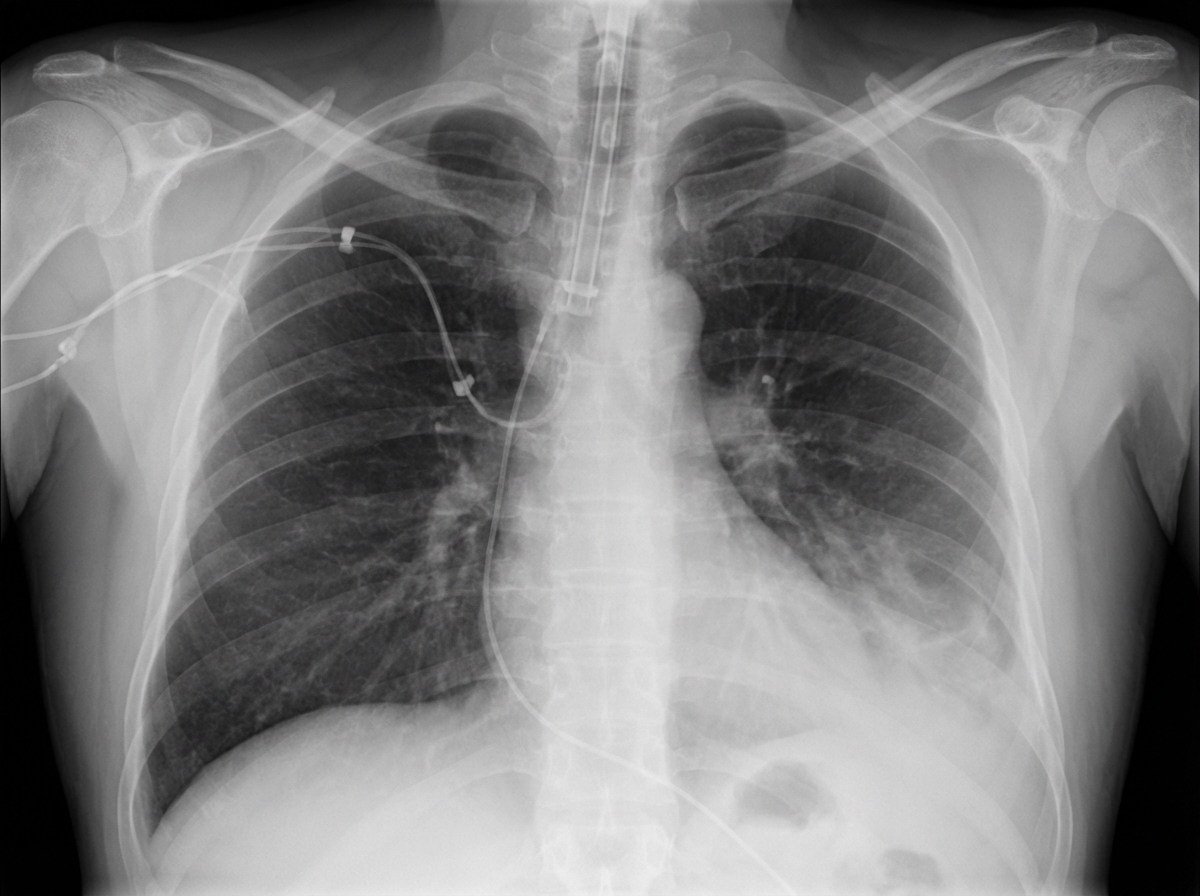
A 27-year-old man is brought to the emergency department 45 minutes after being involved in a motor vehicle collision. He is agitated. He has pain in his upper right arm, which he is cradling in his left arm. His temperature is 36.7°C (98°F), pulse is 135/min, respirations are 25/min, and blood pressure is 145/90 mm Hg. His breathing is shallow. Pulse oximetry on 100% oxygen via a non-rebreather face mask shows an oxygen saturation of 83%. He is confused and oriented only to person. Examination shows multiple bruises on the right anterior thoracic wall. The pupils are equal and reactive to light. On inspiration, his right chest wall demonstrates paradoxical inward movement while his left chest wall is expanding. There is pain to palpation and crepitus over his right anterior ribs. The remainder of the examination shows no abnormalities. An x-ray of the chest is shown. Two large-bore IVs are placed. After fluid resuscitation and analgesia, which of the following is the most appropriate next step in management?
A 27-year-old male presents to the Emergency Room as a code trauma after being shot in the neck. En route, the patient's blood pressure is 127/73 mmHg, pulse is 91/min, respirations are 14/min, and oxygen saturation is 100% on room air with GCS of 15. On physical exam, the patient is in no acute distress; however, there is an obvious entry point with oozing blood near the left lateral neck above the cricoid cartilage with a small hematoma that is non-pulsatile and stable since arrival. The rest of the physical exam is unremarkable. Rapid hemoglobin returns back at 14.1 g/dL. After initial resuscitation, what is the next best step in management?
An 11-year-old boy is brought to the emergency department with sudden and severe pain in the left scrotum that started 2 hours ago. He has vomited twice. He has no dysuria or frequency. There is no history of trauma to the testicles. The temperature is 37.7°C (99.9°F). The left scrotum is swollen, erythematous, and tender. The left testis is elevated and swollen with a transverse lie. The cremasteric reflex is absent. Ultrasonographic examination is currently pending. Which of the following is the most likely diagnosis?
An 18-year-old woman is brought to the emergency department by her coach, 30 minutes after injuring her left knee while playing field hockey. She was tackled from the left side and has been unable to bear weight on her left leg since the accident. She fears the left knee may be unstable upon standing. There is no personal or family history of serious illness. The patient appears uncomfortable. Vital signs are within normal limits. Examination shows a swollen and tender left knee; range of motion is limited by pain. The medial joint line is tender to touch. The patient's hip is slightly flexed and abducted, and the knee is slightly flexed while the patient is in the supine position. Gentle valgus stress is applied across the left knee and medial joint laxity is noted. The remainder of the examination shows no further abnormalities. Which of the following is the most likely diagnosis?
A 52-year-old obese man is brought to the emergency department 30 minutes after he was involved in a high-speed motor vehicle collision. He was the unrestrained driver. On arrival, he is lethargic. His pulse is 112/min, respirations are 10/min and irregular, and blood pressure is 94/60 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 91%. The pupils are equal and react sluggishly to light. He withdraws his extremities to pain. There are multiple bruises over his face, chest, and abdomen. Breath sounds are decreased over the left lung base. Two large bore peripheral venous catheters are inserted and 0.9% saline infusion is begun. Rapid sequence intubation is initiated and endotracheal intubation is attempted without success. Bag and mask ventilation is continued. Pulse oximetry shows an oxygen saturation of 84%. The patient has no advance directive and family members have not arrived. Which of the following is the most appropriate next step in the management of this patient?
A 63-year-old man is brought to the emergency department, 30 minutes after being involved in a high-speed motor vehicle collision. He is obtunded on arrival. He is intubated and mechanical ventilation is begun. The ventilator is set at a FiO2 of 60%, tidal volume of 440 mL, and positive end-expiratory pressure of 4 cm H2O. On the third day of intubation, his temperature is 37.3°C (99.1°F), pulse is 91/min, and blood pressure is 103/60 mm Hg. There are decreased breath sounds over the left lung base. Cardiac examination shows no abnormalities. The abdomen is soft and not distended. Arterial blood gas analysis shows: pH 7.49 pCO2 29 mm Hg pO2 73 mm Hg HCO3- 20 mEq/L O2 saturation 89% Monitoring shows a sudden increase in the plateau airway pressure. An x-ray of the chest shows deepening of the costophrenic angle on the left side. Which of the following is the most appropriate next step in management?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app