
Trauma/Emergencies — MCQs

On this page
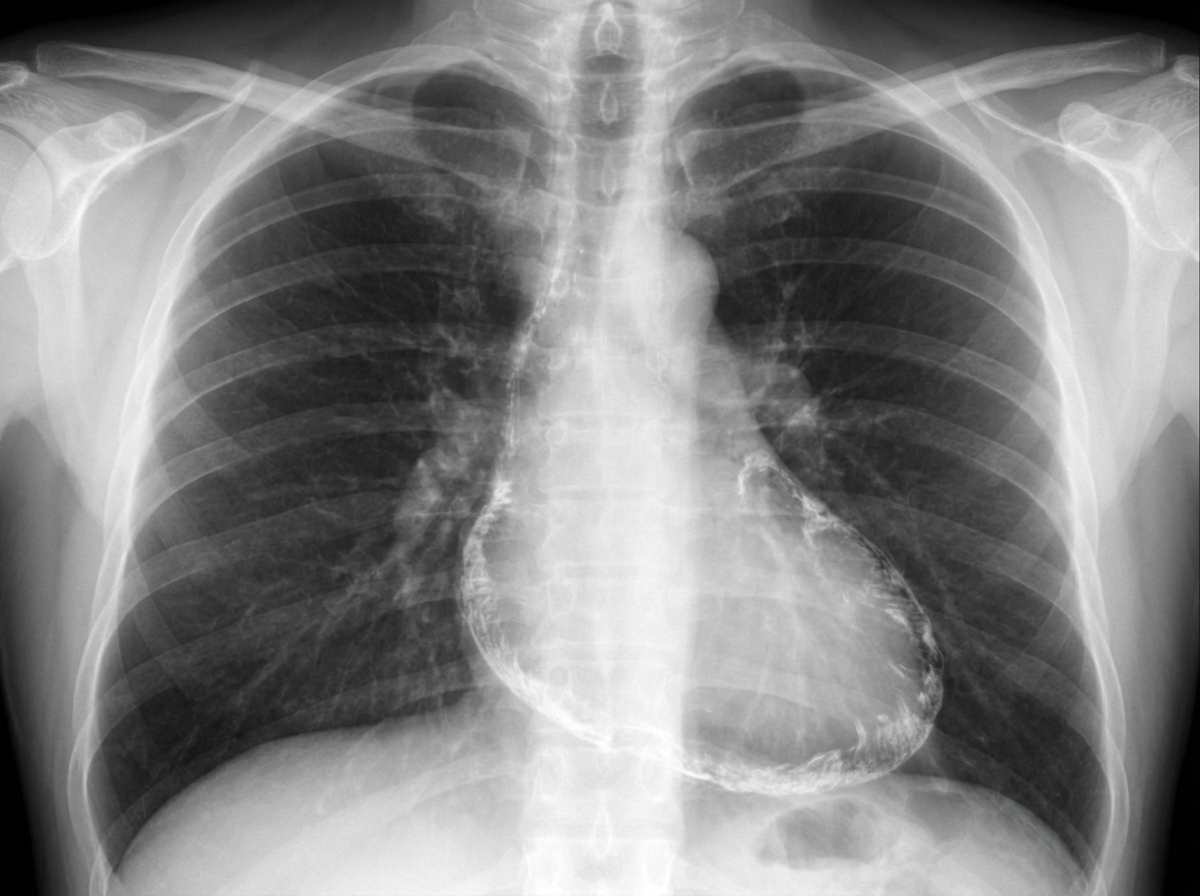
A 52-year-old man presents to the emergency department because of fatigue, abdominal distension, and swelling of both legs for the last 3 weeks. His wife says that he lost some weight recently. He has had type 2 diabetes mellitus for 12 years, for which he takes metformin and sitagliptin. He has a history of Hodgkin’s lymphoma which was successfully treated with mediastinal radiation 20 years ago. He does not smoke or drink alcohol. He has a family history of type 2 diabetes in his father and elder sister. Vital signs include a blood pressure of 100/70 mm Hg, a temperature of 36.9°C (98.4°F), and a regular radial pulse of 90/min. On physical examination, there is jugular venous distension, most prominently when the patient inhales. Bilateral ankle pitting edema is present, and his abdomen is distended with shifting dullness on percussion. An early diastolic knocking sound is audible on the chest. His chest X-ray is shown in the exhibit. Which of the following is the best treatment for this patient?
A previously healthy 64-year-old man comes to the physician 3 days after noticing a lump in his right groin while he was bathing. He has no history of trauma to the region. He has hypercholesterolemia and hypertension treated with atorvastatin and labetalol. He has smoked 2 packs of cigarettes daily for 35 years. His vital signs are within normal limits. Examination shows a 4-cm (1.6-in), nontender, pulsatile mass with a palpable thrill at the right midinguinal point. On auscultation, a harsh continuous murmur is heard over the mass. Femoral and pedal pulses are palpable bilaterally. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
A 62-year-old man presents to the emergency department with sudden onset of severe left leg pain accompanied by numbness and weakness. His medical history is remarkable for hypertension and hyperlipidemia. His vital signs include a blood pressure of 155/92 mm Hg, a temperature of 37.1°C (98.7°F), and an irregular pulse of 92/min. Physical examination reveals absent left popliteal and posterior tibial pulses. His left leg is noticeably cold and pale. There is no significant tissue compromise, nerve damage, or sensory loss. Which of the following will most likely be required for this patient's condition?
A 28-year-old man is brought to the emergency department after being struck by a car an hour ago as he was crossing the street. He did not lose consciousness. He is complaining of pain in his right arm, forehead, and pelvis. He also has the urge to urinate, but has been unable to do so since the accident. He takes no medications. His temperature is 37.1°C (98.9°F), pulse is 72/min, respirations are 18/min, and blood pressure is 118/82 mm Hg. There are abrasions over his scalp and face and a 1x3 cm area of ecchymosis above his right eye. Abdominal examination shows suprapubic tenderness. There is a scant amount of blood at the urethral meatus. There is no cervical spinal tenderness. Musculoskeletal examination shows tenderness and ecchymosis over his right distal forearm. An x-ray of the pelvis shows a fracture of the pelvic ramus. A CT scan of the head and neck show no abnormalities. Which of the following is the best next step in the management of this patient?
A 77-year-old man is brought to the emergency department by his wife because of headache, nausea, and vomiting for 24 hours. His wife says that over the past 2 weeks, he has been more irritable and has had trouble remembering to do routine errands. Two weeks ago, he fell during a skiing accident but did not lose consciousness. He has coronary artery disease and hypertension. He has smoked one pack of cigarettes daily for 50 years. He has had 2 glasses of wine daily since his retirement 10 years ago. Current medications include atenolol, enalapril, furosemide, atorvastatin, and aspirin. He appears acutely ill. He is oriented to person but not to place or time. His temperature is 37°C (98.6°F), pulse is 99/min, respirations are 16/min, and blood pressure is 160/90 mm Hg. During the examination, he is uncooperative and unable to answer questions. Deep tendon reflexes are 4+ on the left and 2+ on the right. Babinski's sign is present on the left. There is mild weakness of the left iliopsoas and hamstring muscles. A CT scan of the head without contrast shows a high-density, 15-mm crescentic collection across the right hemispheric convexity. Which of the following is the most appropriate next step in the management of this patient?
A 27-year-old man is brought to the emergency department after a motor vehicle accident. He was the unrestrained driver in a head on collision. The patient is responding incoherently and is complaining of being in pain. He has several large lacerations and has been impaled with a piece of metal. IV access is unable to be obtained and a FAST exam is performed. His temperature is 98.2°F (36.8°C), blood pressure is 90/48 mmHg, pulse is 150/min, respirations are 13/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
A 24-year-old man is brought by ambulance to the emergency department after a motor vehicle accident. He was the front seat driver in a head on collision. He is currently unconscious. The patient’s past medical history is only notable for an allergy to amoxicillin as he developed a rash when it was given for a recent upper respiratory infection 1 week ago. Otherwise, he is a college student in good health. The patient is resuscitated. A FAST exam is notable for free fluid in Morrison’s pouch. An initial assessment demonstrates only minor bruises and scrapes on his body. After further resuscitation the patient becomes responsive and begins vomiting. Which of the following is the most likely diagnosis?
A 27-year-old man presents to the emergency department after being stabbed. The patient was robbed at a local pizza parlor and was stabbed over 10 times with a large kitchen knife with an estimated 7 inch blade in the ventral abdomen. His temperature is 97.6°F (36.4°C), blood pressure is 74/54 mmHg, pulse is 180/min, respirations are 19/min, and oxygen saturation is 98% on room air. The patient is intubated and given blood products and vasopressors. Physical exam is notable for multiple stab wounds over the patient's abdomen inferior to the nipple line. Which of the following is the best next step in management?
A 25-year-old man presents with pain and a limited range of motion in his right shoulder. He is a collegiate baseball player and says he has not been playing for approx. 1 week because his shoulder hurts when he throws. He also noticed trouble raising his arm over his head. He describes the pain as moderate, dull, and aching in character and worse when he moves his arm above his shoulder or when he lays in bed on his side. He denies any recent acute trauma to the shoulder or other joint pain. The medical history is significant for asthma, which is managed medically. The current medications include albuterol inhaled and fluticasone. He reports a 5-year history of chewing tobacco but denies smoking, alcohol, or drug use. The temperature is 37.0°C (98.6°F); blood pressure is 110/85 mm Hg; pulse is 97/min; respiratory rate is 15/min, and oxygen saturation is 99% on room air. The physical examination is significant for tenderness to palpation on the anterolateral aspect of the right shoulder. The active range of motion on abduction of the right shoulder is decreased. The passive range of motion is intact. No swelling, warmth, or erythema is noted. The sensation is intact. The deep tendon reflexes are 2+ bilaterally. The peripheral pulses are 2+. The laboratory results are all within normal limits. A plain radiograph of the right shoulder shows no evidence of fracture or bone deformities. An MRI of the right shoulder shows increased T1 and T2 signals in the rotator cuff tendon. Which of the following is the best initial course of treatment for this patient?
A 23-year-old man presents to the emergency department with testicular pain. His symptoms started 15 minutes ago and have not improved on the ride to the hospital. The patient’s past medical history is non-contributory, and he is not currently taking any medications. His temperature is 98.5°F (36.9°C), blood pressure is 123/62 mmHg, pulse is 124/min, respirations are 18/min, and oxygen saturation is 98% on room air. Physical exam is notable for a non-tender abdomen. The patient’s right testicle appears higher than his left and is held in a horizontal position. Stroking of the patient’s medial thigh elicits no response. Which of the following is the best treatment for this patient?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app