
Trauma/Emergencies — MCQs

On this page
A 38-year-old man is brought to the emergency department 35 minutes after he sustained a gunshot wound to the right thigh. He has type 1 diabetes mellitus. On arrival, his pulse is 112/min, respirations are 20/min, and blood pressure is 115/69 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. There is an entrance wound on the anteromedial surface of the right thigh 2 cm below the inguinal ligament. There is no bruit or thrill. There is no exit wound. The pedal pulse is diminished on the right side compared to the left. The abdomen is soft and nontender. The remainder of the examination shows no abnormalities. Laboratory studies show: Hematocrit 46% Serum Urea nitrogen 24 mg/dL Glucose 160 mg/dL Creatinine 3.1 mg/dL Which of the following is the most appropriate next step in management?
A 15-year-old boy presents with a sore throat and difficulty swallowing. The patient says he has had a sore throat over the last 3 weeks. Two days ago it became acutely more painful. There is no significant past medical history nor current medications. The vital signs include: temperature 38.2°C (100.8°F), blood pressure 100/70 mm Hg, pulse 101/min, respiratory rate 26/min, and oxygen saturation 99% on room air. Physical examination reveals an inability to fully open his mouth (trismus) and drooling. The patient's voice has a muffled quality. CT of the head is significant for the findings seen in the picture. Which of the following is the best initial course of treatment for this patient?

A 52-year-old woman is brought to the emergency department by fire and rescue after being involved in a motor vehicle accident. The paramedics report that the patient’s car slipped off the road during a rainstorm and rolled into a ditch. The patient was restrained and the airbags deployed during the crash. The patient has a past medical history of hypertension, hyperlipidemia, hypothyroidism, and gout. Her home medications include hydrochlorothiazide, simvastatin, levothyroxine, and allopurinol. The patient is alert on the examination table. Her temperature is 98.2°F (36.8°C), blood pressure is 83/62 mmHg, pulse is 131/min, respirations are 14/min, and SpO2 is 96%. She has equal breath sounds in all fields bilaterally. Her skin is cool with diffuse bruising over her abdomen and superficial lacerations, and her abdomen is diffusely tender to palpation. She is moving all four extremities equally. The patient’s FAST exam is equivocal. She is given several liters of intravenous fluid during her trauma evaluation but her blood pressure does not improve. Which of the following is the best next step?
A 27-year-old man comes to the physician because of pain and swelling in his right knee that began 3 days ago when he fell during football practice. He fell on his flexed right knee as he dove to complete a pass. He felt some mild knee pain but continued to practice. Over the next 2 days, the pain worsened and the knee began to swell. Today, the patient has an antalgic gait. Examination shows a swollen and tender right knee; flexion is limited by pain. The right knee is flexed and pressure is applied to proximal tibia; 8 mm of backward translation of the foreleg is observed. Which of the following is most likely injured?
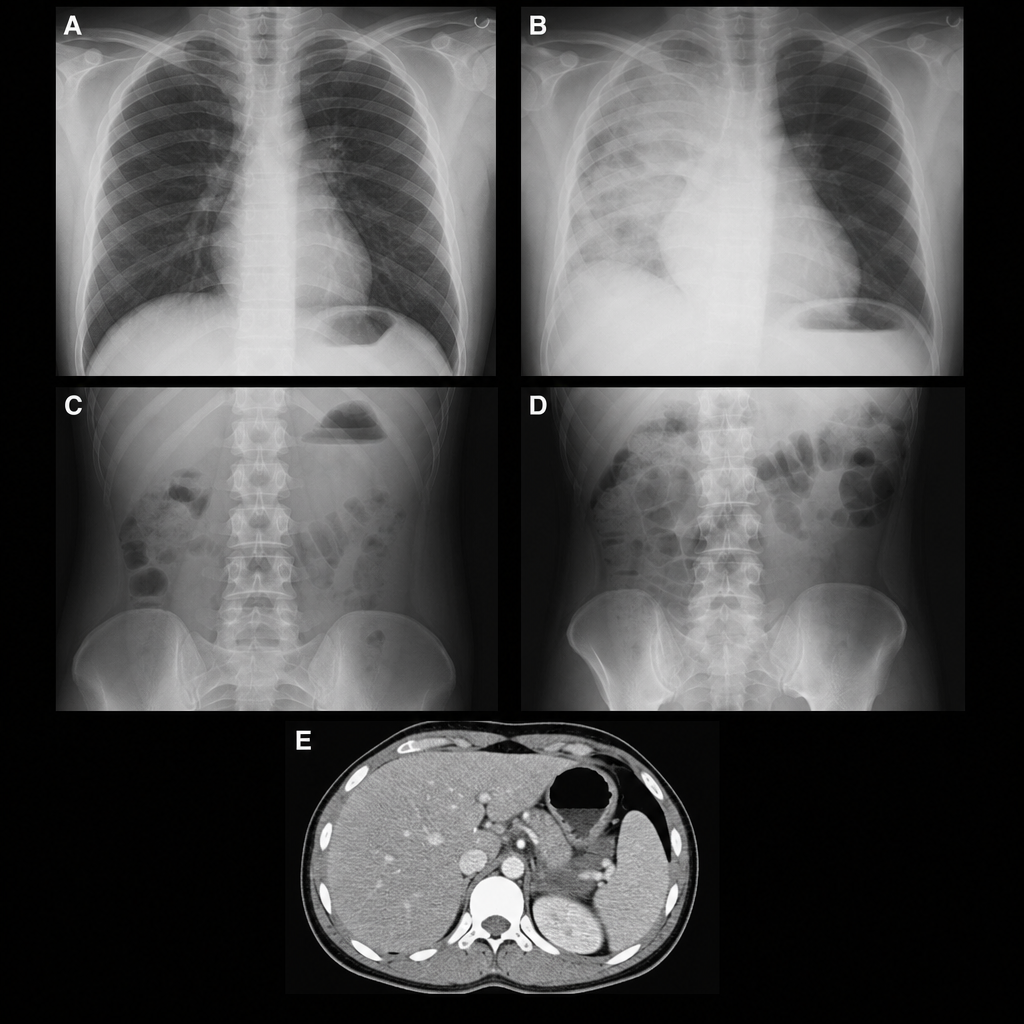
A 24-year-old male is brought in by fire rescue after being the restrained driver in a motor vehicle accident. There was a prolonged extraction. At the scene, the patient was GCS 13. The patient was boarded and transported. In the trauma bay, vitals are T 97.2°F, HR 132 bpm, BP 145/90 mmHg, RR 22/min, and O2 Sat 100%. ABCs are intact with a GCS of 15, and on secondary survey you note left lower rib tenderness and ecchymosis over the left upper quadrant. FAST exam is positive at Morison's pouch. Abdominal exam shows exquisite tenderness to palpation with rebound and guarding. Which of the following images demonstrates the injury most likely present in this patient?
A 24-year-old woman presents to her primary care physician for unilateral breast pain. The patient states that she has been breastfeeding her son but has been experiencing worsening pain recently. Her pain is severe enough that she is now struggling to breastfeed her son with her left breast. The patient's past medical history is notable for gestational diabetes which was controlled with diet and exercise. Her temperature is 101°F (38.3°C), blood pressure is 137/69 mmHg, pulse is 100/min, respirations are 13/min, and oxygen saturation is 97% on room air. Physical exam reveals an erythematous breast with a 3-cm tender and fluctuant mass of the left breast. Which of the following is the best next step in management?
A 40-year-old woman who works as a secretary presents to your office complaining of new pain and numbness in both of her hands. For the past few weeks, the sensation has occurred after long days of typing, but it now occasionally wakes her up from sleep. You do not note any deformities of her wrists or hands, but you are able to reproduce pain and numbness in the first three and a half digits by tapping the wrist. What is the best initial treatment for this patient's complaint?
A 32-year-old man is brought to the emergency department 15 minutes after falling 7 feet onto a flat-top wooden post. On arrival, he is in severe pain and breathing rapidly. His pulse is 135/min, respirations are 30/min, and blood pressure is 80/40 mm Hg. There is an impact wound in the left fourth intercostal space at the midaxillary line. Auscultation shows tracheal deviation to the right and absent breath sounds over the left lung. There is dullness to percussion over the left chest. Neck veins are flat. Cardiac examination shows no abnormalities. Two large-bore intravenous catheters are placed and intravenous fluid resuscitation is begun. Which of the following is the most likely diagnosis?
A 35-year-old man is brought into the emergency department by emergency medical services with his right hand wrapped in bloody bandages. The patient states that he is a carpenter and was cutting some wood for a home renovation project when he looked away and injured one of his digits with a circular table saw. He states that his index finger was sliced off and is being brought in by his wife. On exam, his vitals are within normal limits and stable, and he is missing part of his second digit on his right hand distal to the proximal interphalangeal joint. How should the digit be transported to the hospital for the best outcome?
A 35-year-old man is brought to the emergency department 20 minutes after being involved in a motor vehicle collision in which he was a restrained passenger. The patient is confused. His pulse is 140/min and blood pressure is 85/60 mm Hg. Examination shows a hand-sized hematoma on the anterior chest wall. An ECG shows sinus tachycardia. Which of the following structures is most likely injured in this patient?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app