
Trauma/Emergencies — MCQs

On this page
A 67-year-old man is brought to the emergency room after being involved in a traffic accident. He currently complains of bilateral hip pain. His vital signs are within the normal range, and he is hemodynamically stable. The pelvic compression test is positive. External genitalia appears normal, except there is blood at the urethral meatus and a contusion at the base of the scrotum. Digital rectal examination (DRE) shows a high-riding ballotable prostate. An X-ray reveals the presence of a pelvic fracture. Which of the following initial actions is the most appropriate for this patient?
A 34-year-old woman is brought into the emergency department by emergency medical services after an electrical fire in her apartment. She is coughing with an O2 saturation of 98%, on 2L of nasal cannula. The patient's physical exam is significant for a burn on her right forearm that appears to be dry, white, and leathery in texture. Her pulses and sensations are intact in all extremities. The patient's vitals are HR 110, BP 110/80, T 99.2, RR 20. She has no evidence of soot in her mouth and admits to leaving the room as soon as the fire started. Which of the following is the best treatment for this patient?
A 45-year-old gentleman comes to his primary care physician complaining of redness and foul-smelling discharge from his penis. The patient is not married and denies sexual activity. Upon further questioning, he denies trauma or any associated fevers or chills. After the initial work-up was found to be negative for sexually-transmitted diseases, a biopsy and imaging were ordered. The biopsy shows squamous cell carcinoma (SCC). Which of the following is associated with a reduced risk of developing penile SCC?
A 27-year-old woman is brought to the emergency department after sustaining a fall from her bicycle 1 hour ago. The patient was on her way to work as she lost her balance, hitting her head on the sidewalk. She had an initial loss of consciousness for a couple of minutes following the accident. She currently has nausea and a headache. She has vomited twice during the last 30 minutes. She has no history of a serious illness. The patient does not smoke or drink alcohol. She has never used illicit drugs. She takes no medications. Her temperature is 37°C (98.6°F), pulse is 50/min, respirations are 10/min, and blood pressure is 160/90 mm Hg. She is oriented to person, place, and time. Her lungs are clear to auscultation. Cardiac examination shows bradycardia but no murmurs, rubs, or gallops. The abdomen is soft and nontender. There is a bruise on the right temporal side of the head. While performing the remainder of the physical examination the patient starts having a seizure. Intravenous lorazepam is administered and she is admitted to the intensive care unit. Which of the following is the most likely diagnosis in this patient?
Ultrasonography of the scrotum shows a 2-cm hypoechoic, homogeneous testicular mass with sharp margins. A CT scan of the abdomen shows a single enlarged para-aortic lymph node. Which of the following is the most appropriate next step in management?
A 25-year-old man presents to the emergency department after a motor vehicle collision. He was an unrestrained driver in a head on collision. The patient has a Glasgow coma scale of 9 and is responding to questions inappropriately. His temperature is 96.0°F (35.6°C), blood pressure is 64/44 mmHg, pulse is 192/min, respirations are 32/min, and oxygen saturation is 94% on room air. Which of the following interventions is the best treatment for this patient’s hypotension?
A 55-year-old woman comes to the physician 10 days after noticing a mass in her left breast while bathing. She is concerned that it is breast cancer because her sister was diagnosed with breast cancer 3 years ago at 61 years of age. Menopause occurred 6 months ago. She has smoked 2 packs of cigarettes daily for 30 years. She took an oral contraceptive for 20 years. Current medications include hormone replacement therapy and a calcium supplement. Examination shows a 2.5-cm, palpable, hard, nontender, mass in the upper outer quadrant of the left breast; there is tethering of the skin over the lump. Examination of the right breast and axillae shows no abnormalities. Mammography shows an irregular mass with microcalcifications and oil cysts. A core biopsy shows foam cells and multinucleated giant cells. Which of the following is the most appropriate next step in management?
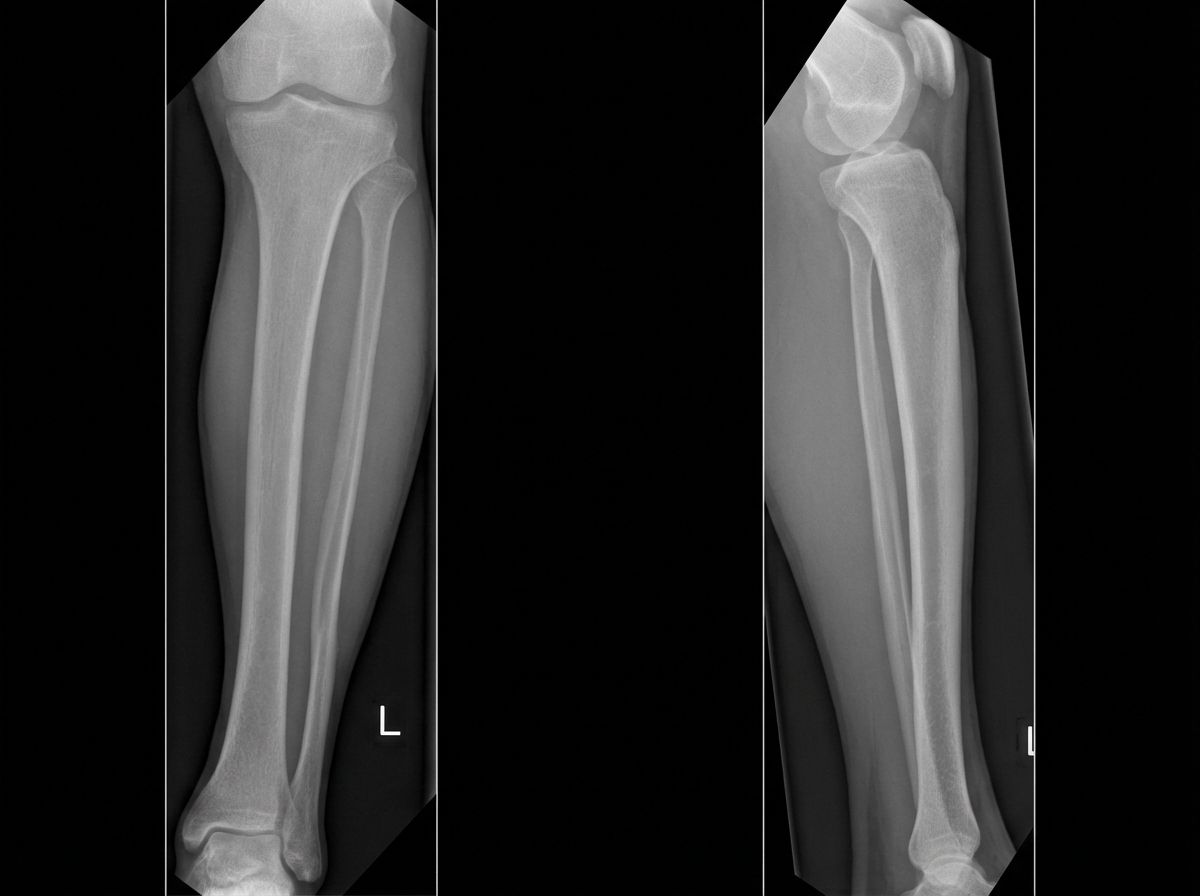
A 36-year-old man comes to the emergency department 4 hours after a bike accident for severe pain and swelling in his right leg. He has not had a headache, nausea, vomiting, abdominal pain, or blood in his urine. He has a history of gastroesophageal reflux disease and allergic rhinitis. He has smoked one pack of cigarettes daily for 17 years and drinks an average of one alcoholic beverage daily. His medications include levocetirizine and pantoprazole. He is in moderate distress. His temperature is 37°C (98.6°F), pulse is 112/min, and blood pressure is 140/80 mm Hg. Examination shows multiple bruises over both lower extremities and the face. There is swelling surrounding a 2 cm laceration 13 cm below the right knee. The lower two-thirds of the tibia is tender to palpation and the skin is pale and cool to the touch. The anterior tibial, posterior tibial, and dorsalis pedis pulses are weak. Capillary refill time of the right big toe is 4 seconds. Dorsiflexion of his right foot causes severe pain in his calf. Cardiopulmonary examination is normal. An x-ray is ordered, which is shown below. Which of the following is the most appropriate next step in management?
A 6-year-old girl is brought to the emergency department because of right elbow swelling and pain 30 minutes after falling onto her outstretched right arm. She has been unable to move her right elbow since the fall. Physical examination shows bruising, swelling, and tenderness of the right elbow; range of motion is limited by pain. An x-ray of the right arm shows a supracondylar fracture of the humerus with posterior displacement of the distal fragment. Further evaluation is most likely to show which of the following findings?
A 56-year-old man is brought to the emergency department 25 minutes after he was involved in a high-speed motor vehicle collision where he was the unrestrained passenger. He has severe lower abdominal and pelvic pain. On arrival, he is alert and oriented. His pulse is 95/min, respirations are 22/min, and blood pressure is 106/62 mm Hg. Examination shows severe tenderness to palpation over the lower abdomen and over the left anterior superior iliac spine. There is no limb length discrepancy. Application of downward pressure over the pelvis shows no springy resistance or instability. Rectal examination is unremarkable. A focused assessment with sonography shows no free fluid in the abdomen. There is no blood at the urethral meatus. Placement of a Foley catheter shows gross hematuria. An x-ray of the pelvis shows a fracture of the left pelvic edge. Which of the following is the most appropriate next step in management?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app