
Trauma/Emergencies — MCQs

On this page
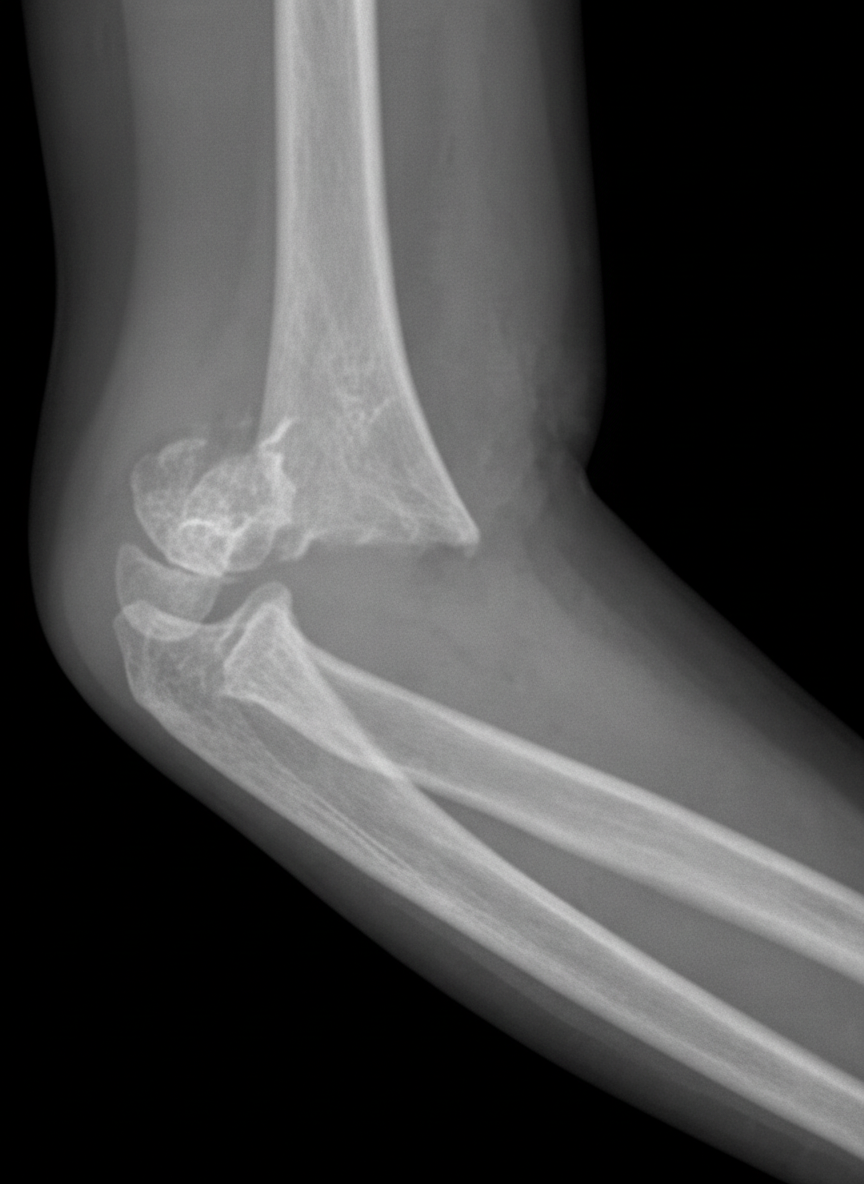
A 5-year-old boy is brought to the emergency department for right elbow swelling and pain 45 minutes after he fell while playing on the monkey bars during recess. He has been unable to move his right elbow since the fall. Examination shows ecchymosis, swelling, and tenderness of the right elbow; range of motion is limited by pain. The remainder of the examination shows no abnormalities. An x-ray of the right arm is shown. Which of the following is the most likely complication of this patient's injury?
A 54-year-old man comes to the physician because of a painful mass in his left thigh for 3 days. He underwent a left lower limb angiography for femoral artery stenosis and had a stent placed 2 weeks ago. He has peripheral artery disease, coronary artery disease, hypercholesterolemia and type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for 34 years. Current medications include enalapril, aspirin, simvastatin, metformin, and sitagliptin. His temperature is 36.7°C (98°F), pulse is 88/min, and blood pressure is 116/72 mm Hg. Examination shows a 3-cm (1.2-in) tender, pulsatile mass in the left groin. The skin over the area of the mass shows no erythema and is cool to the touch. A loud bruit is heard on auscultation over this area. The remainder of the examination shows no abnormalities. Results of a complete blood count and serum electrolyte concentrations show no abnormalities. Duplex ultrasonography shows an echolucent sac connected to the common femoral artery, with pulsatile and turbulent blood flow between the artery and the sac. Which of the following is the most appropriate next best step in management?
A 45-year-old man is brought to the emergency department following a house fire. Following initial stabilization, the patient is transferred to the ICU for management of his third-degree burn injuries. On the second day of hospitalization, a routine laboratory panel is obtained, and the results are demonstrated below. Per the nurse, he remains stable compared to the day prior. His temperature is 99°F (37°C), blood pressure is 92/64 mmHg, pulse is 98/min, respirations are 14/min, and SpO2 is 98%. A physical examination demonstrates an unresponsive patient with extensive burn injuries throughout his torso and lower extremities. Hemoglobin: 13 g/dL Hematocrit: 36% Leukocyte count: 10,670/mm^3 with normal differential Platelet count: 180,000/mm^3 Serum: Na+: 135 mEq/L Cl-: 98 mEq/L K+: 4.7 mEq/L HCO3-: 25 mEq/L BUN: 10 mg/dL Glucose: 123 mg/dL Creatinine: 1.8 mg/dL Thyroid-stimulating hormone: 4.3 µU/mL Triiodothyronine: 48 ng/dL Thyroxine: 10 ug/dL Ca2+: 8.7 mg/dL AST: 89 U/L ALT: 135 U/L What is the best course of management for this patient?
A 22-year-old man comes to the physician because of a progressive swelling and pain in his right ring finger for the past 2 days. The pain began while playing football, when his finger got caught in the jersey of another player who forcefully pulled away. Examination shows that the right ring finger is extended. There is pain and swelling at the distal interphalangeal joint. When the patient is asked to make a fist, his right ring finger does not flex at the distal interphalangeal joint. There is no joint laxity. Which of the following is the most likely diagnosis?
A 25-year-old woman is brought to the emergency department after being involved in a rear-end collision, in which she was the restrained driver of the back car. On arrival, she is alert and active. She reports pain in both knees and severe pain over the right groin. Temperature is 37°C (98.6°F), pulse is 116/min, respirations are 19/min, and blood pressure is 132/79 mm Hg. Physical examination shows tenderness over both knee caps. The right groin is tender to palpation. The right leg is slightly shortened, flexed, adducted, and internally rotated. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
A 76-year-old man is brought to the emergency room because of one episode of epistaxis. His pulse is 110/min. Physical examination shows pallor; there is blood in the oral cavity. Examination of the nasal cavity with a nasal speculum shows active bleeding from the posterior nasal cavity. Tamponade with a balloon catheter is attempted without success. The most appropriate next step in the management is ligation of a branch of a vessel of which of the following arteries?
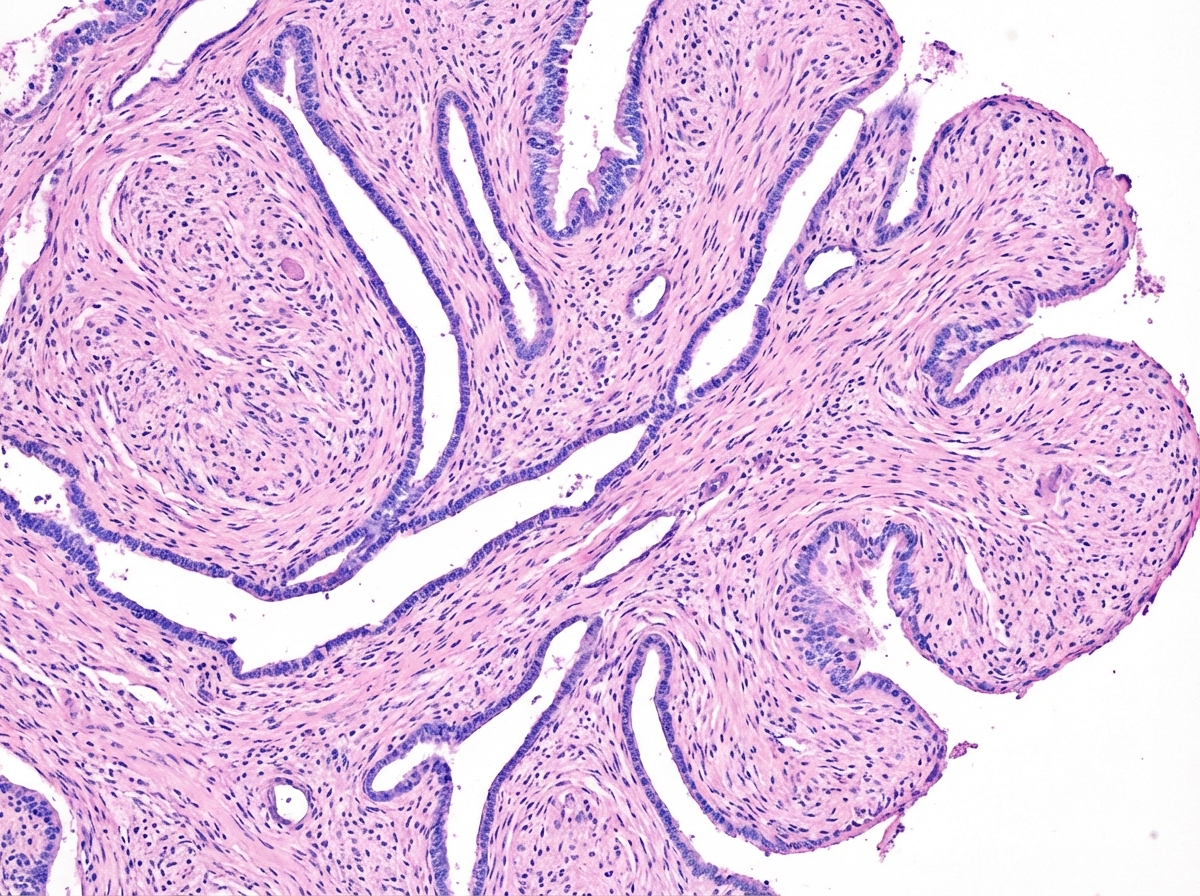
A 48-year-old woman comes to the physician for the evaluation of a left breast mass that she noticed 4 weeks ago. It has rapidly increased in size during this period. Vital signs are within normal limits. Examination shows large dense breasts; a 6-cm, nontender, multinodular mass is palpated in the upper outer quadrant of the left breast. There are no changes in the skin or nipple. There is no palpable cervical or axillary adenopathy. Mammography shows a smooth polylobulated mass. An image of a biopsy specimen is shown. Which of the following is the most likely diagnosis?
A 22-year-old man is rushed to the emergency department after a motor vehicle accident. The patient states that he feels weakness and numbness in both of his legs. He also reports pain in his lower back. His airway, breathing, and circulation is intact, and he is conversational. Neurologic exam is significant for bilateral lower extremity flaccid paralysis and impaired pain and temperature sensation up to T10-T11 with normal vibration sense. A computerized tomography scan of the spine is performed which shows a vertebral burst fracture of the vertebral body at the level of T11. Which of the following findings is most likely present in this patient?
A 61-year-old woman presents to her physician with a persistent cough. She has been unable to control her cough and also is finding it increasingly difficult to breathe. The cough has been persistent for about 2 months now, but 2 weeks ago she started noticing streaks of blood in the sputum regularly after coughing. Over the course of 4 months, she has also observed an unusual loss of 10 kg (22 lb) in her weight. She has an unchanged appetite and remains fairly active, which makes her suspicious as to the cause of her weight loss. Another troublesome concern for her is that on a couple occasions over the past few weeks, she has observed herself drenched in sweat when she wakes up in the morning. Other than having a 35 pack-year smoking history, her medical history is insignificant. She is sent for a chest X-ray which shows a central nodule of about 13 mm located in the hilar region. Which of the following would be the next best step in the management of this patient?
A 67-year-old woman has fallen from the second story level of her home while hanging laundry. She was brought to the emergency department immediately and presented with severe abdominal pain. The patient is anxious, and her hands and feet feel very cold to the touch. There is no evidence of bone fractures, superficial skin wounds, or a foreign body penetration. Her blood pressure is 102/67 mm Hg, respirations are 19/min, pulse is 87/min, and temperature is 36.7°C (98.0°F). Her abdominal exam reveals rigidity and severe tenderness. A Foley catheter and nasogastric tube are inserted. The central venous pressure (CVP) is 5 cm H2O. The medical history is significant for hypertension. Which of the following is best indicated for the evaluation of this patient?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app