
Trauma/Emergencies — MCQs

On this page
A 68-year-old man is brought to the emergency department because of fever, progressive weakness, and cough for the past five days. He experienced a similar episode 2 months ago, for which he was hospitalized for 10 days while visiting his son in Russia. He states that he has never fully recovered from that episode. He felt much better after being treated with antibiotics, but he still coughs often during meals. He sometimes also coughs up undigested food after eating. For the last 5 days, his coughing has become more frequent and productive of yellowish-green sputum. He takes hydrochlorothiazide for hypertension and pantoprazole for the retrosternal discomfort that he often experiences while eating. He has smoked half a pack of cigarettes daily for the last 30 years and drinks one shot of vodka every day. The patient appears thin. His temperature is 40.1°C (104.2°F), pulse is 118/min, respirations are 22/min, and blood pressure is 125/90 mm Hg. Auscultation of the lungs shows right basal crackles. There is dullness on percussion at the right lung base. The remainder of the physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 15.4 g/dL Leukocyte count 17,000/mm3 Platelet count 350,000/mm3 Na+ 139 mEq/L K+ 4.6 mEq/L Cl- 102 mEq/L HCO3- 25 mEq/L Urea Nitrogen 16 mg/dL Creatinine 1.3 mg/dL An x-ray of the chest shows a right lower lobe infiltrate. Which of the following is the most likely explanation for this patient's symptoms?
A 23-year-old woman presents to her primary care physician for knee pain. The pain started yesterday and has not improved since then. The patient is generally in good health. She attends college and plays soccer for her school's team. Three days ago, she was slide tackled during a game and her leg was struck from the inside. She fell to the ground and sat out for the rest of the game. It was not until yesterday that she noticed swelling in her knee. She also feels as if her knee is unstable and does not feel confident bearing weight on her leg during athletic activities. Her past medical history is notable for asthma, which is currently treated with an albuterol inhaler. On physical exam, you note bruising over her leg, knee, and medial thigh, and edema of her knee. Passive range of motion of the knee is notable only for minor clicking and catching of the joint. The patient's gait appears normal, though the patient states that her injured knee does not feel stable. Further physical exam is performed and imaging is ordered. Which of the following is the most likely diagnosis?
A 56-year-old man is brought to the emergency department after falling 16 feet from a ladder. He has severe pain in both his legs and his right arm. He appears pale and diaphoretic. His temperature is 37.5°C (99.5°F), pulse is 120/min and weak, respirations are 26/min, and blood pressure is 80/50 mm Hg. He opens his eyes and withdraws in response to painful stimuli and makes incomprehensible sounds. The abdomen is soft and nontender. All extremities are cold, with 1+ pulses distally. Arterial blood gas analysis on room air shows: pH 7.29 PCO2 33 mm Hg PO2 65 mm Hg HCO3- 15 mEq/L A CT scan shows displaced fractures of the pelvic ring, as well as fractures of both tibiae, the right distal radius, and right proximal humerus. The patient undergoes emergent open reduction and is admitted to the intensive care unit. Which of the following best indicates inadequate fluid resuscitation?
A 22-year-old man is brought to the emergency department because of progressive left-sided scrotal pain for 4 hours. He describes the pain as throbbing in nature and 6 out of 10 in intensity. He has vomited once on the way to the hospital. He has had pain during urination for the past 4 days. He has been sexually active with 2 female partners over the past year and uses condoms inconsistently. His father was diagnosed with testicular cancer at the age of 51 years. He appears anxious. His temperature is 36.9°C (98.42°F), pulse is 94/min, and blood pressure is 124/78 mm Hg. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and nontender. Examination shows a tender, swollen left testicle and an erythematous left hemiscrotum. Urine dipstick shows leukocyte esterase; urinalysis shows WBCs. Which of the following is the most appropriate next step in management?
A 35-year-old man is referred to a physical therapist due to limitation of movement in the wrist and fingers of his left hand. He cannot hold objects or perform daily activities with his left hand. He broke his left arm at the humerus one month ago. The break was simple and treatment involved a cast for one month. Then he lost his health insurance and could not return for follow up. Only after removing the cast did he notice the movement issues in his left hand and wrist. His past medical history is otherwise insignificant, and vital signs are within normal limits. On examination, the patient’s left hand is pale and flexed in a claw-like position. It is firm and tender to palpation. Right radial pulse is 2+ and left radial pulse is 1+. The patient is unable to actively extend his fingers and wrist, and passive extension is difficult and painful. Which of the following is a proper treatment for the presented patient?
A 20-year-old man presents to the family medicine clinic with left knee pain. He is the star running back for his college football team with a promising future in the sport. He states he injured his knee 2 days ago during the final game of the season while making a cutting move, where his foot was planted and rotated outward and his knee buckled inward. He admits to feeling a ‘pop’ and having immediate pain. He denies any locking, clicking, or giving way since the event. Physical examination reveals an antalgic gait with avoidance of active knee extension. His left knee demonstrates moderate, diffuse swelling and is very tender to palpation along the joint line. Which of the following structures is most likely damaged in this patient?
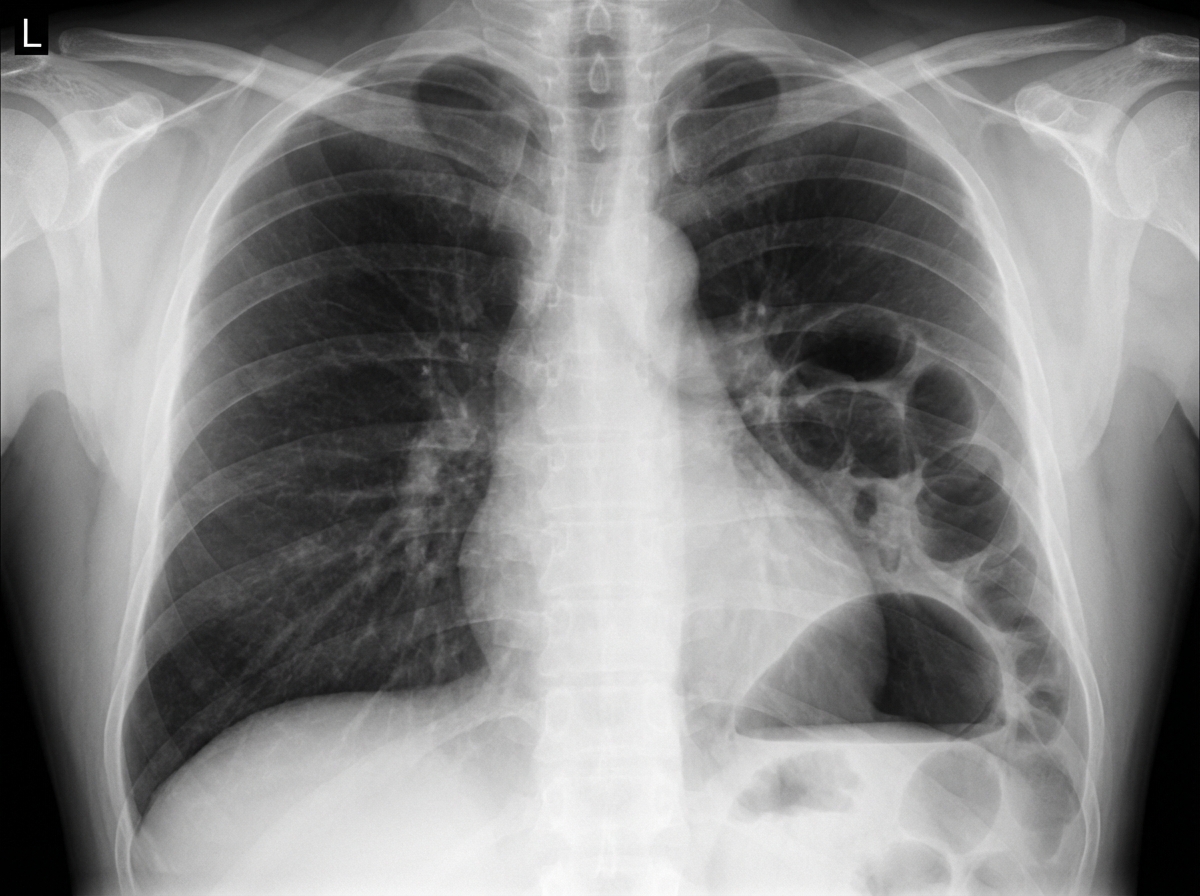
A 28-year-old man is brought to the emergency department with shortness of breath and chest pain, 35 minutes after he was involved in a high-speed motor vehicle collision. He was the helmeted driver of a scooter hit by a truck. On arrival, he is alert and oriented with a Glasgow Coma Scale rating of 14. His temperature is 37.3°C (99.1°F), pulse is 103/min, respirations are 33/min and blood pressure is 132/88 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 94%. Examination shows multiple abrasions over his abdomen and extremities. There is a 2.5-cm (1-in) laceration on the left side of the chest. There are decreased breath sounds over the left base. Cardiac examination shows no abnormalities. The abdomen is soft and there is tenderness to palpation over the left upper quadrant. Bowel sounds are normal. His hemoglobin concentration is 13.6 g/dL, leukocyte count is 9,110/mm3, and platelet count is 190,000/mm3. A chest x-ray is shown. Which of the following is the most likely diagnosis?
An 8-year-old boy and his 26-year-old babysitter are brought into the emergency department with severe injuries caused by a motor vehicle accident. The child is wheeled to the pediatric intensive care unit with a severe injury to his right arm, as well as other external and internal injuries. He is hemorrhaging and found to be hemodynamically unstable. He subsequently requires transfusion and surgery, and he is currently unconscious. The pediatric trauma surgeon evaluates the child’s arm and realizes it will need to be amputated at the elbow. Which of the following is the most appropriate course of action to take with regards to the amputation?
A 37-year-old man is brought to the emergency department by a friend after he was found lying unconscious outside his front door. The friend reports that they were “pretty drunk” the previous night, and she had dropped her friend off at his home and driven off. When she came back in the morning, she found him passed out on the ground next to the doorstep. On arrival, he is conscious and cooperative. He reports feeling cold, with severe pain in his hands and face. He remembers having lost his gloves last night. His rectal temperature is 35.2°C (95.3°F), pulse is 86/min, respirations are 17/min, and blood pressure is 124/58 mm Hg. Examination shows decreased sensations over the distal fingers, which are cold to touch. The skin over the distal phalanges is cyanotic, hard, waxy, and tender, with surrounding edema. Laboratory studies are within the reference range. An x-ray of the chest and ECG show no abnormalities. Which of the following is the most appropriate next step in management?
A 35-year-old man is brought to the emergency department 40 minutes after spilling hot oil over himself in a kitchen accident. Examination shows multiple tense blisters over the abdomen, anterior chest, and right upper extremity. On deroofing the blisters, the skin over the right upper extremity is tender, pink, and blanches with pressure. The skin over the abdomen and anterior chest is tender, mottled, and does not blanch with pressure. The left thigh shows erythema only, is tender, and shows quick capillary refill after blanching with pressure. Which of the following most closely approximates the body surface area affected by 2nd-degree burns in this patient?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app