
Trauma/Emergencies — MCQs

On this page
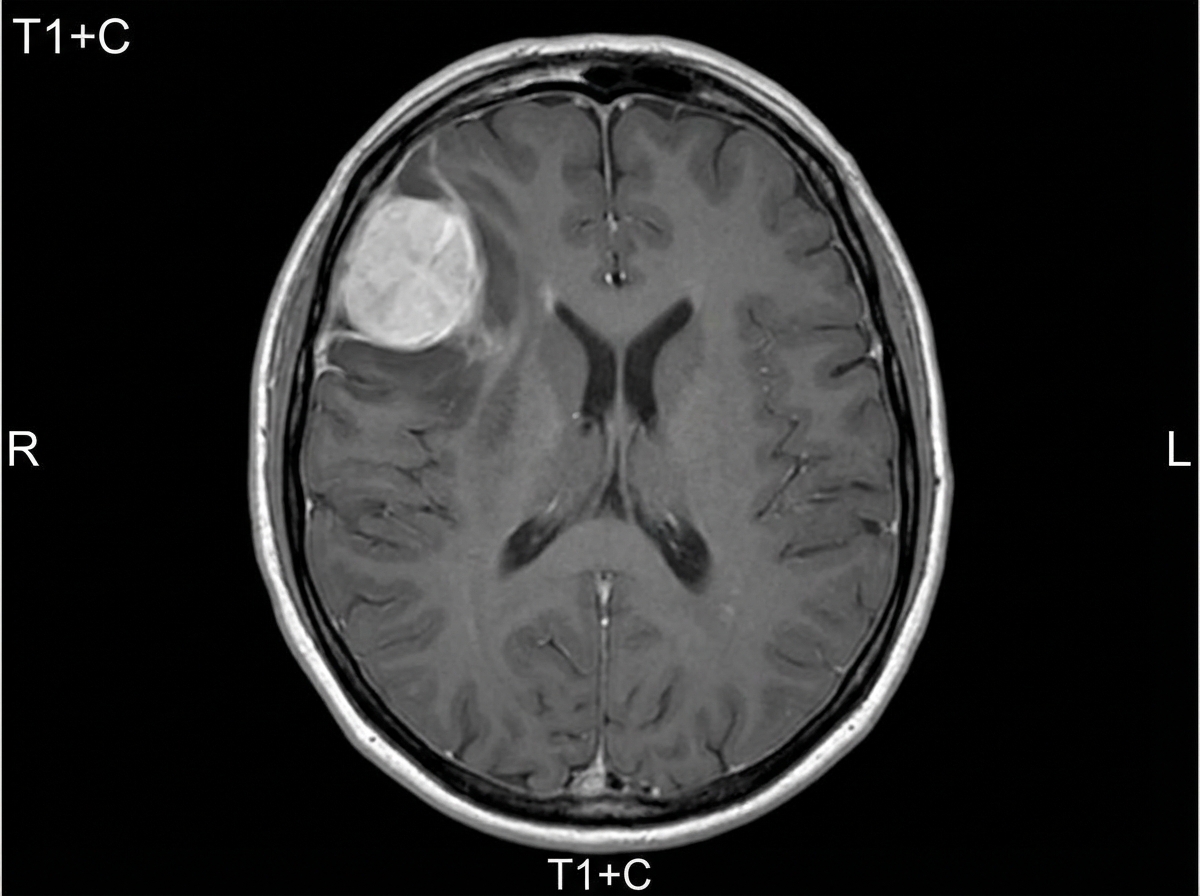
A 54-year-old woman comes to the physician because of paresthesias and weakness in her left leg for one year. Her symptoms have become progressively worse during this period and have led to some difficulty walking for the past month. She has had frequent headaches for the past 4 months. She has a history of hypertension and hypothyroidism. Current medications include amlodipine and levothyroxine. Her temperature is 37.3°C (99.1°F), pulse is 97/min, and blood pressure is 110/80 mm Hg. Neurologic examination shows decreased muscle strength in the left lower extremity. Deep tendon reflexes of the lower extremity are 4+ on the left and 2+ on the right side. The remainder of the examination shows no abnormalities. A complete blood count and serum concentrations of electrolytes, glucose, creatinine, and calcium are within the reference ranges. An MRI of the brain is shown. Which of the following is the most appropriate next step in management?
A 23-year-old man is brought to the emergency department because of severe right shoulder pain and inability to move the shoulder for the past 30 minutes. The pain began after being tackled while playing football. He has nausea but has not vomited. He is in no apparent distress. Examination shows the right upper extremity externally rotated and slightly abducted. Palpation of the right shoulder joint shows tenderness and an empty glenoid fossa. The right humeral head is palpated below the coracoid process. The left upper extremity is unremarkable. The radial pulses are palpable bilaterally. Which of the following is the most appropriate next step in management?
A 35-year-old man is brought to the emergency department 30 minutes after being involved in a motor vehicle collision. The patient was on his way to work before he lost control of his car and crashed into a tree. On arrival, the patient appears weak and lethargic. He has pain in his abdomen. His temperature is 37°C (98.6°F), pulse is 121/min, respirations are 22/min, and blood pressure is 85/60 mm Hg. He is oriented to person but not to place or time. The lungs are clear to auscultation. Cardiac examination shows tachycardia but no murmurs, rubs, or gallops. Abdominal examination shows several bruises above the umbilicus; there is diffuse abdominal tenderness. Focused assessment with sonography in trauma (FAST) is performed but the results are inconclusive. In addition to intravenous fluid resuscitation, which of the following is the most appropriate next step in management of this patient?
A 17-year-old male presents to the emergency department after a knife fight. He initially refused to come to the hospital, but one of his wounds overlying the right antecubital fossa would not stop bleeding. Vitals include: BP 90/65, HR 115, and RR 24. He reports that he is light-headed and having visual changes. You hold direct pressure over the wound on his right arm while the rest of the team resuscitates him with crystalloid and pRBCs. After his vitals signs normalize, you note that his right arm is cool and you are unable to palpate a radial pulse. The vascular surgery team explores his right arm, finding and repairing a lacerated brachial artery. Two hours post-operatively he is complaining of 10/10 pain in his right forearm and screams out loud when you passively move his fingers. What is the most appropriate next step in management?
An 18-year-old man presents to the emergency department after an automobile accident. His vitals have significantly dropped since admission. Upon examination, his abdomen is slightly distended, the ribs on the right side are tender and appear broken, and breath sounds are diminished at the base of the right lung. An abdominal ultrasound and chest X-ray are ordered. Ultrasound shows fluid in the abdominal cavity and trauma to the liver. X-ray confirmed broken ribs and pleural effusion on the right. Based on these findings, the surgeons recommend immediate surgery. Upon entering the abdomen, an exsanguinating hemorrhage is observed. The Pringle maneuver is used to reduce bleeding. What was clamped during this maneuver?
A 33-year-old man is brought to the emergency department 20 minutes after losing control over his bicycle and colliding with a parked car. The handlebar of the bicycle hit his lower abdomen. On arrival, he is alert and oriented. His pulse is 90/min, respirations are 17/min and blood pressure is 110/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 97%. The pupils are equal and reactive to light. There are multiple bruises over his chest and lower extremities. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. There is no pelvic instability. Rectal examination is unremarkable. A complete blood count, prothrombin time, and serum concentrations of glucose, creatinine, and electrolytes are within the reference range. Urine dipstick is mildly positive for blood. Microscopic examination of the urine shows 20 RBCs/hpf. Which of the following is the most appropriate next step in management?
A 22-year-old man comes to the emergency department for pain and swelling of his left knee one day after injuring it while playing soccer. While sprinting on the field, he slipped as he attempted to kick the ball and landed on the anterior aspect of his knee. He underwent an appendectomy at the age of 16 years. His vitals signs are within normal limits. Examination shows a swollen and tender left knee; range of motion is limited by pain. The tibial tuberosity shows tenderness to palpation. The left tibia is displaced posteriorly when force is applied to the proximal tibia after flexing the knee. The remainder of the examination shows no abnormalities. An x-ray of the left knee joint shows an avulsion fracture of the tibial condyle. Which of the following is the most likely diagnosis?
A 65-year-old man comes to the emergency department because of sudden, worsening pain in his right calf and foot that started 30 minutes ago. He also has a tingling sensation and weakness in his right leg. He has had no similar episodes, recent trauma, or claudication. He has type 2 diabetes mellitus and was diagnosed with hypertension 20 years ago. His sister has systemic sclerosis. He works as an office administrator and sits at his desk most of the day. He has smoked one and a half packs of cigarettes daily for 30 years. Current medications include metformin and lisinopril. His pulse is 110/min, respirations are 16/min, and blood pressure is 140/90 mm Hg. His right leg is pale and cool to touch. Muscle strength in his right leg is mildly reduced. Pedal pulses are absent on the right. Which of the following is the most likely underlying cause of this patient's symptoms?
Three hours later, the patient is reassessed. Her right arm is put in an elevated position and physical examination of the extremity is performed. The examination reveals reduced capillary return and peripheral pallor. Pulse oximetry of her right index finger on room air shows an oxygen saturation of 84%. Which of the following is the most appropriate next step in management?
A 67-year-old man comes to the emergency department because of decreased vision and black spots in front of his left eye for the past 24 hours. He states that it feels as if 'a curtain is hanging over his eye.' He sees flashes of light intermittently. He has no pain or diplopia. He underwent cataract surgery on the left eye 2 weeks ago. He has hypertension and type 2 diabetes mellitus. His sister has open-angle glaucoma. Current medications include metformin, linagliptin, ramipril, and hydrochlorothiazide. Vital signs are within normal limits. Examination shows a visual acuity in the right eye of 20/25 and the ability to count fingers at 3 feet in the left eye. The pupils are equal and reactive. The corneal reflex is present. The anterior chamber shows no abnormalities. The confrontation test is normal on the right side and shows nasal and inferior defects on the left side. Cardiopulmonary examination shows no abnormalities. The patient is awaiting dilation for fundus examination. Which of the following is the most likely diagnosis?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app