
Trauma/Emergencies — MCQs

On this page
A 72-year-old man comes to the physician for a 5-month history of hoarseness, exertional dyspnea, and fatigue. He does not smoke or drink alcohol. His pulse is 98/min and irregular. His voice is coarse in quality. Physical examination shows a liver span of 16 cm and a soft diastolic murmur heard best at the apex. Which of the following is the most likely cause of this patient's hoarseness?
A 33-year-old man presents to his primary care physician with shoulder pain. He states that he can't remember a specific instance when the injury occurred. He is a weight lifter and competes in martial arts. The patient has no past medical history and is currently taking a multivitamin. Physical exam demonstrates pain with abduction of the patient's right shoulder and with external rotation of the right arm. There is subacromial tenderness with palpation. His left arm demonstrates 10/10 strength with abduction as compared to 4/10 strength with abduction of the right arm. Which of the following best confirms the underlying diagnosis?
A 17-year-old boy is brought to the emergency department by his parents 6 hours after he suddenly began to experience dyspnea and pleuritic chest pain at home. He has a remote history of asthma in childhood but has not required any treatment since the age of four. His temperature is 98.4°F (36.9°C), blood pressure is 100/76 mmHg, pulse is 125/min, respirations are 24/min. On exam, he has decreased lung sounds and hyperresonance in the left upper lung field. A chest radiograph shows a slight tracheal shift to the right. What is the best next step in management?
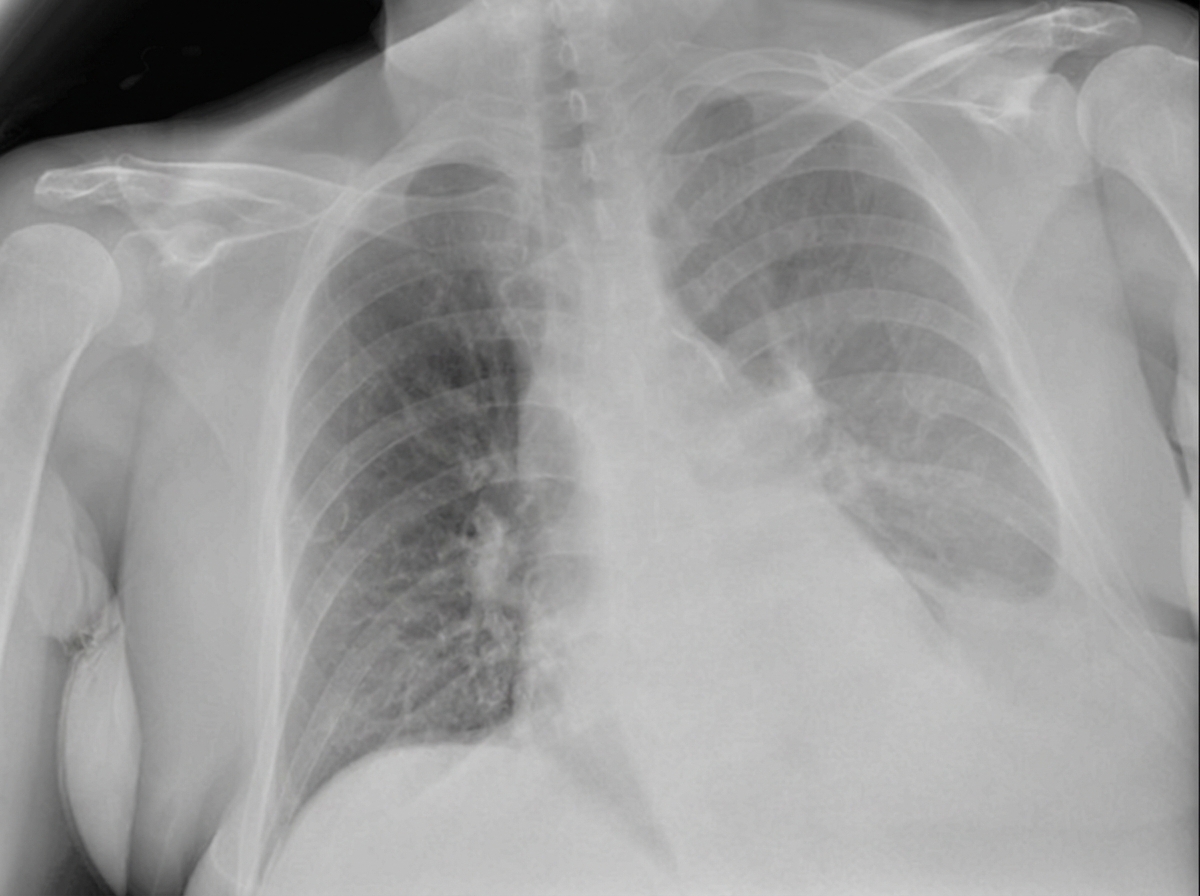
A 27-year-old soldier is brought to the emergency department of a military hospital 20 minutes after being involved in a motor vehicle accident during a training exercise. He was an unrestrained passenger. On arrival, he has shortness of breath and chest pain. He appears pale and anxious. His temperature is 37°C (98.6°F), pulse is 110/min, respirations are 20/min, and blood pressure is 100/65 mm Hg. He is alert and oriented to person, place, and time. Examination shows pale conjunctivae and mucous membranes. There is bruising on the chest, extremities, and abdomen. The lungs show diminished breath sounds on the left. He has normal heart sounds and flat neck veins. The abdomen is flat, soft, and mildly tender. The remainder of the physical examination shows no abnormalities. High-flow oxygen is applied, and intravenous fluid resuscitation is begun. A chest x-ray is obtained. Which of the following is the most appropriate next step in management?
A 32-year-old man is brought to the emergency department 10 minutes after he sustained a stab wound to the left chest just below the clavicle. On arrival, he is hypotensive with rapid and shallow breathing and appears anxious and agitated. He is intubated and mechanically ventilated. Infusion of 0.9% saline is begun. Five minutes later, his pulse is 137/min and blood pressure is 84/47 mm Hg. Examination shows a 3-cm single stab wound to the left chest at the 4th intercostal space at the midclavicular line without active external bleeding. Cardiovascular examination shows muffled heart sounds and jugular venous distention. Breath sounds are normal bilaterally. Further evaluation of this patient is most likely to show which of the following findings?
A 37-year-old man presents to the emergency department after he cut his hand while working on his car. The patient has a past medical history of antisocial personality disorder and has been incarcerated multiple times. His vitals are within normal limits. Physical exam is notable for a man covered in tattoos with many bruises over his face and torso. Inspection of the patient's right hand reveals 2 deep lacerations on the dorsal aspects of the second and third metacarpophalangeal (MCP) joints. The patient is given a tetanus vaccination, and the wound is irrigated. Which of the following is appropriate management for this patient?
A 45-year-old man presents to an urgent care clinic because he coughed up blood this morning. Although he had a persistent cough for the past 3 weeks, he had never coughed up blood until now. His voice is hoarse and admits that it has been like that for the past few months. Both his past medical history and family history are insignificant. He has smoked a pack of cigarettes a day since the age of 20 and drinks wine every night before bed. His vitals are: heart rate of 78/min, respiratory rate of 14/min, temperature of 36.5°C (97.8°F), blood pressure of 140/88 mm Hg. An indirect laryngoscopy reveals a rough vegetating lesion on the free border of the right vocal cord. Which of the following is the most likely diagnosis?
A 22-year-old soldier sustains a stab wound to his chest during a military attack in Mali. He is brought to the combat medic by his unit for a primary survey. The soldier reports shortness of breath. He is alert and oriented to time, place, and person. His pulse is 99/min, respirations are 32/min, and blood pressure is 112/72 mm Hg. Examination shows a 2-cm wound at the left fourth intercostal space at the midclavicular line. Bubbling of blood is seen with each respiration at the wound site. There is no jugular venous distention. There is hyperresonance to percussion and decreased breath sounds on the left side. The trachea is at the midline. Which of the following is the most appropriate next step in management?
A 65-year-old man with a past medical history of anterior myocardial infarction, peripheral arterial disease, and known patent foramen ovale presents to the emergency department after being found down from a fall on the sidewalk in the middle of winter. He states that his right leg feels numb and painful at the same time. He insists that he did not slip on ice or snow, yet fell suddenly. He is taking aspirin, simvastatin, and cilastazol. Vital signs show T 98.0 F, BP 100/60, HR 100, RR 18. His pulse is irregularly irregular. His right leg appears pale with no dorsalis pedis and posterior tibial pulses compared to 2+ pulses on the left. He cannot discern soft or sharp touch in his right leg. Which intervention will most likely improve the viability of this patient's right leg?
A 60-year-old man is brought to the emergency department 25 minutes after falling and hitting his left flank on a concrete block. He has severe left-sided chest pain and mild shortness of breath. He underwent a right knee replacement surgery 2 years ago. He has type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for 42 years. Current medications include metformin, sitagliptin, and a multivitamin. He appears uncomfortable. His temperature is 37.5°C (99.5°F), pulse is 102/min, respirations are 17/min, and blood pressure is 132/90 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Examination shows multiple abrasions on his left flank and trunk. The upper left chest wall is tender to palpation and bony crepitus is present. There are decreased breath sounds over both lung bases. Cardiac examination shows no murmurs, rubs, or gallops. The abdomen is soft and nontender. Focused assessment with sonography for trauma is negative. An x-ray of the chest shows nondisplaced fractures of the left 4th and 5th ribs, with clear lung fields bilaterally. Which of the following is the most appropriate next step in management?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app