
Trauma/Emergencies — MCQs

On this page
A 40-year-old male visits a urologist and reports that for the past 2 weeks, his penis has been gradually curving to the right with associated pain during intercourse. He is able to have a normal erection and he does not recollect of any trauma to his penis. Although he is married, he admits to having unprotected sexual relationship with several females in the past year. His vitals are normal and physical examination is unremarkable except for a lesionless curved penis. It is painless to touch. Test results for sexually transmitted disease is pending. Which of the following is the most likely cause?
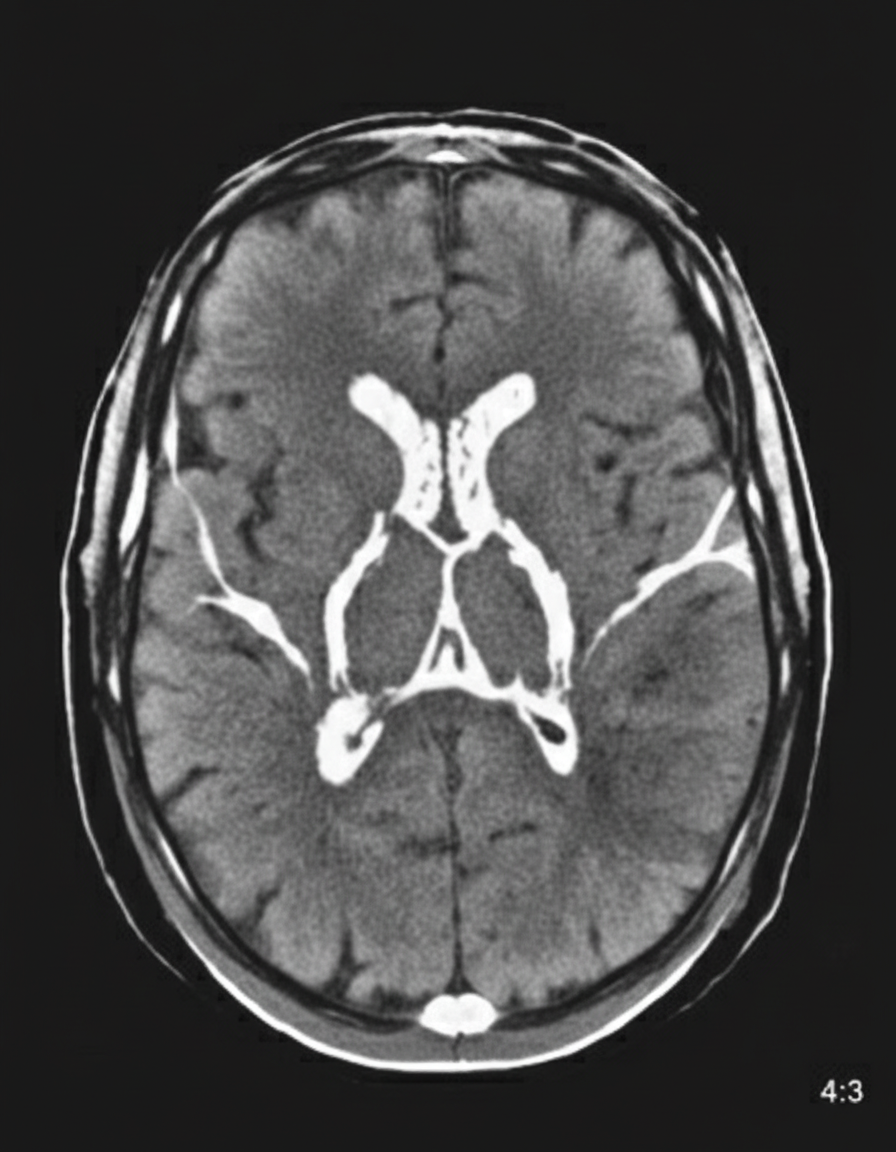
A 48-year-old woman is brought to the emergency department because of a 1-hour history of sudden-onset headache associated with nausea and vomiting. The patient reports she was sitting at her desk when the headache began. The headache is global and radiates to her neck. She has hypertension. She has smoked one pack of cigarettes daily for the last 10 years. She drinks alcohol occasionally. Her father had a stroke at the age 58 years. Current medications include hydrochlorothiazide. She is in severe distress. She is alert and oriented to person, place, and time. Her temperature is 38.2°C (100.8°F), pulse is 89/min, respirations are 19/min, and blood pressure is 150/90 mm Hg. Cardiopulmonary examination shows no abnormalities. Cranial nerves II–XII are intact. She has no focal motor or sensory deficits. She flexes her hips and knees when her neck is flexed while lying in a supine position. A CT scan of the head is shown. Subsequent CT angiography reveals a wide-necked middle cerebral artery aneurysm at the MCA bifurcation. Which of the following is the most appropriate intervention?
A 23-year-old man comes to the emergency department with an open wound on his right hand. He states that he got into a bar fight about an hour ago. He appears heavily intoxicated and does not remember the whole situation, but he does recall lying on the ground in front of the bar after the fight. He does not recall any history of injuries but does remember a tetanus shot he received 6 years ago. His temperature is 37°C (98.6°F), pulse is 77/min, and blood pressure is 132/78 mm Hg. Examination shows a soft, nontender abdomen. His joints have no bony deformities and display full range of motion. There is a 4-cm (1.6-in) lesion on his hand with the skin attached only on the ulnar side. The wound, which appears to be partly covered with soil and dirt, is irrigated and debrided by the hospital staff. Minimal erythema and no purulence is observed in the area surrounding the wound. What is the most appropriate next step in management?
A 43-year-old man is brought to the emergency department 40 minutes after falling off a 10-foot ladder. He has severe pain and swelling of his right ankle and is unable to walk. He did not lose consciousness after the fall. He has no nausea. He appears uncomfortable. His temperature is 37°C (98.6°F), pulse is 98/min, respirations are 16/min, and blood pressure is 110/80 mm Hg. He is alert and oriented to person, place, and time. Examination shows multiple abrasions over both lower extremities. There is swelling and tenderness of the right ankle; range of motion is limited by pain. The remainder of the examination shows no abnormalities. An x-ray of the ankle shows an extra-articular calcaneal fracture. Intravenous analgesia is administered. Which of the following is the most appropriate next step in the management of this patient?
A 27-year-old woman presents to her family physician with pain on the front of her right knee. The pain started 2 months ago after she began training for a marathon, and it was gradual in onset and has slowly worsened. The pain increases with prolonged sitting and climbing stairs. She denies significant knee trauma. Her only medication is diclofenac sodium as needed for pain. Medical history is unremarkable. The vital signs include: temperature 36.9°C (98.4°F), blood pressure 100/70 mm Hg, and heart rate 78/min. Her body mass index is 26 kg/m2. The pain is reproduced by applying direct pressure to the right patella, and there is increased patellar laxity with medial and lateral displacement. The remainder of the examination is otherwise unremarkable. Which of the following is the most likely diagnosis?
A 27-year-old man presents to the emergency department after he was assaulted and shot during a robbery. The patient was beaten with a baseball bat and has a bullet entry wound in his neck. He is currently complaining of diffuse pains but is able to speak. His voice sounds muffled, and he is requesting pain medications. An initial resuscitation is begun in the trauma bay. The patient's general appearance reveals ecchymosis throughout his body and minor scrapes and cuts, and possible multiple facial bone fractures. There is another bullet wound found in the left side of his back without an exit wound. Which of the following is the best next step in management?
A 36-year-old man was sent to the Emergency Department after a stray baseball hit him in the left eye during a game. Paramedics on sight could not perform the necessary testing and encouraged the patient to visit an ED for further testing and imaging. At the Emergency Department, the patient complains of slight pain in the orbital region and minimal diplopia that mildly increases with upward gaze. The patient’s blood pressure is 110/60 mm Hg, heart rate is 53/min, respiratory rate is 13/min, and temperature 36.6℃ (97.9℉). On physical examination, the patient is alert and responsive. There is an ecchymosis involving the lower lid and infraorbital area on the left side, with a slight downward deviation of the left globe, and conjunctival injection of the left eye. An upward gaze is limited on the left side. The visual acuity is 5/20 bilaterally. A head and neck CT shows a small (0.4 cm), nondisplaced, linear fracture of the left orbital floor. Which of the following statements about the condition the patient presents with is the most accurate?
A 28-year-old woman is brought to the emergency department 30 minutes after being involved in a high-speed motor vehicle collision in which she was the unrestrained driver. On arrival, she is semiconscious and incoherent. She has shortness of breath and is cyanotic. Her pulse is 112/min, respirations are 59/min, and blood pressure is 128/89 mm Hg. Examination shows a 3-cm (1.2-in) laceration on the forehead and multiple abrasions over the thorax and abdomen. There is crepitation on palpation of the thorax on the right. Auscultation of the lung shows decreased breath sounds on the right side. A crunching sound synchronous with the heartbeat is heard best over the precordium. There is dullness on percussion of the right hemithorax. The lips and tongue have a bluish discoloration. There is an open femur fracture on the left. The remainder of the examination shows no abnormalities. Arterial blood gas analysis on room air shows: pH 7.31 PCO2 55 mm Hg PO2 42 mm Hg HCO3- 22 mEq/L O2 saturation 76% The patient is intubated and mechanically ventilated. Infusion of 0.9% saline is begun. Which of the following is the most likely diagnosis?
A 27-year-old soldier stationed in Libya sustains a shrapnel injury during an attack, causing a traumatic above-elbow amputation. The resulting arterial bleed is managed with a tourniquet prior to transport to the military treatment facility. On arrival, he is alert and oriented to person, place, and time. His armor and clothing are removed. His pulse is 145/min, respirations are 28/min, and blood pressure is 95/52 mm Hg. Pulmonary examination shows symmetric chest rise. The lungs are clear to auscultation. Abdominal examination shows no abnormalities. There are multiple shrapnel wounds over the upper and lower extremities. A tourniquet is in place around the right upper extremity; the right proximal forearm has been amputated. One large-bore intravenous catheter is placed in the left antecubital fossa. Despite multiple attempts, medical staff is unable to establish additional intravenous access. Which of the following is the most appropriate next step in management?
A 31-year-old man presents to the Emergency Department with severe left leg pain and paresthesias 4 hours after his leg got trapped by the closing door of a bus. Initially, he had a mild pain which gradually increased to unbearable levels. Past medical history is noncontributory. In the Emergency Department, his blood pressure is 130/80 mm Hg, heart rate is 87/min, respiratory rate is 14/min, and temperature is 36.8℃ (98.2℉). On physical exam, his left calf is firm and severely tender on palpation. The patient cannot actively dorsiflex his left foot, and passive dorsiflexion is limited. Posterior tibial and dorsalis pedis pulses are 2+ in the right leg and 1+ in the left leg. Axial load does not increase the pain. Which of the following is the best next step in the management of this patient?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app