
Trauma/Emergencies — MCQs

On this page
A 66-year-old man is brought to the emergency department after a motor vehicle accident. The patient was a restrained passenger in a car that was struck on the passenger side while crossing an intersection. In the emergency department, he is alert and complaining of abdominal pain. He has a history of hyperlipidemia, gastroesophageal reflux disease, chronic kidney disease, and perforated appendicitis for which he received an interval appendectomy four years ago. His home medications include rosuvastatin and lansoprazole. His temperature is 99.2°F (37.3°C), blood pressure is 120/87 mmHg, pulse is 96/min, and respirations are 20/min. He has full breath sounds bilaterally. He is tender to palpation over the left 9th rib and the epigastrium. He is moving all four extremities. His FAST exam reveals fluid in Morrison's pouch. This patient is most likely to have which of the following additional signs or symptoms?
An obese 52-year-old man is brought to the emergency department because of increasing shortness of breath for the past 8 hours. Two months ago, he noticed a mass on the right side of his neck and was diagnosed with laryngeal cancer. He has smoked two packs of cigarettes daily for 27 years. He drinks two pints of rum daily. He appears ill. He is oriented to person, place, and time. His temperature is 37°C (98.6°F), pulse is 111/min, respirations are 34/min, and blood pressure is 140/90 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 89%. Examination shows a 9-cm, tender, firm subglottic mass on the right side of the neck. Cervical lymphadenopathy is present. His breathing is labored and he has audible inspiratory stridor but is able to answer questions. The lungs are clear to auscultation. Arterial blood gas analysis on room air shows: pH 7.36 PCO2 45 mm Hg PO2 74 mm Hg HCO3- 25 mEq/L He has no advanced directive. Which of the following is the most appropriate next step in management?
A 33-year-old man is brought to the emergency department because of trauma from a motor vehicle accident. His pulse is 122/min and rapid and thready, the blood pressure is 78/37 mm Hg, the respirations are 26/min, and the oxygen saturation is 90% on room air. On physical examination, the patient is drowsy, with cold and clammy skin. Abdominal examination shows ecchymoses in the right flank. The external genitalia are normal. No obvious external wounds are noted, and the rest of the systemic examination values are within normal limits. Blood is sent for laboratory testing and urinalysis shows 6 RBC/HPF. Hematocrit is 22% and serum creatinine is 1.1 mg/dL. Oxygen supplementation and IV fluid resuscitation are started immediately, but the hypotension persists. The focused assessment with sonography in trauma (FAST) examination shows a retroperitoneal fluid collection. What is the most appropriate next step in management?
A 23-year-old patient presents to the emergency department after a motor vehicle accident. The patient was an unrestrained driver involved in a head-on collision. The patient is heavily intoxicated on what he claims is only alcohol. An initial trauma assessment is performed, and is notable for significant bruising of the right forearm. The patient is in the trauma bay, and complains of severe pain in his right forearm. A physical exam is performed and is notable for pallor, decreased sensation, and cool temperature of the skin of the right forearm. Pain is elicited upon passive movement of the right forearm and digits. A thready radial pulse is palpable. A FAST exam is performed, and is negative for signs of internal bleeding. The patient's temperature is 99.5°F (37.5°C), pulse is 100/min, blood pressure is 110/70 mmHg, respirations are 12/min, and oxygen saturation is 98% on room air. Radiography of the right forearm is ordered. The patient is still heavily intoxicated. Which of the following is the best next step in management?
A 3-year-old boy is brought to a respiratory specialist. The family physician referred the child because of recurrent respiratory infections over the past 2 years. Chest X-rays showed a lesion of < 2 cm that includes glands and cysts in the upper lobe of the right lung. Diseases affecting the immune system were investigated and ruled out. No family history of any pulmonary disease or congenital malformations exists. He was born at full term via a normal vaginal delivery with an APGAR score of 10. Which of the following should be highly considered for effective management of this child’s condition?
A 23-year-old woman comes to the emergency department for the evaluation of mild retrosternal pain for the last 7 hours after several episodes of self-induced vomiting. The patient was diagnosed with bulimia nervosa 9 months ago. Her only medication is citalopram. She is 170 cm (5 ft 7 in) tall and weighs 62 kg (136.6 lb); BMI is 21.5 kg/m2. She appears pale. Her temperature is 37°C (98.6°F), pulse is 75/min, respirations are 21/min, and blood pressure is 110/75 mm Hg. The lungs are clear to auscultation. Cardiac examinations shows no murmurs, rubs, or gallops. The abdomen is soft and nontender with no organomegaly. The remainder of the physical examination shows swelling of the salivary glands, dry skin, and brittle nails. An ECG and an x-ray of the chest show no abnormalities. Contrast esophagram with gastrografin shows mild leakage of contrast from the lower esophagus into the mediastinum without contrast extravasation into the pleural and peritoneal cavities. Which of the following is the most appropriate next step in the management?
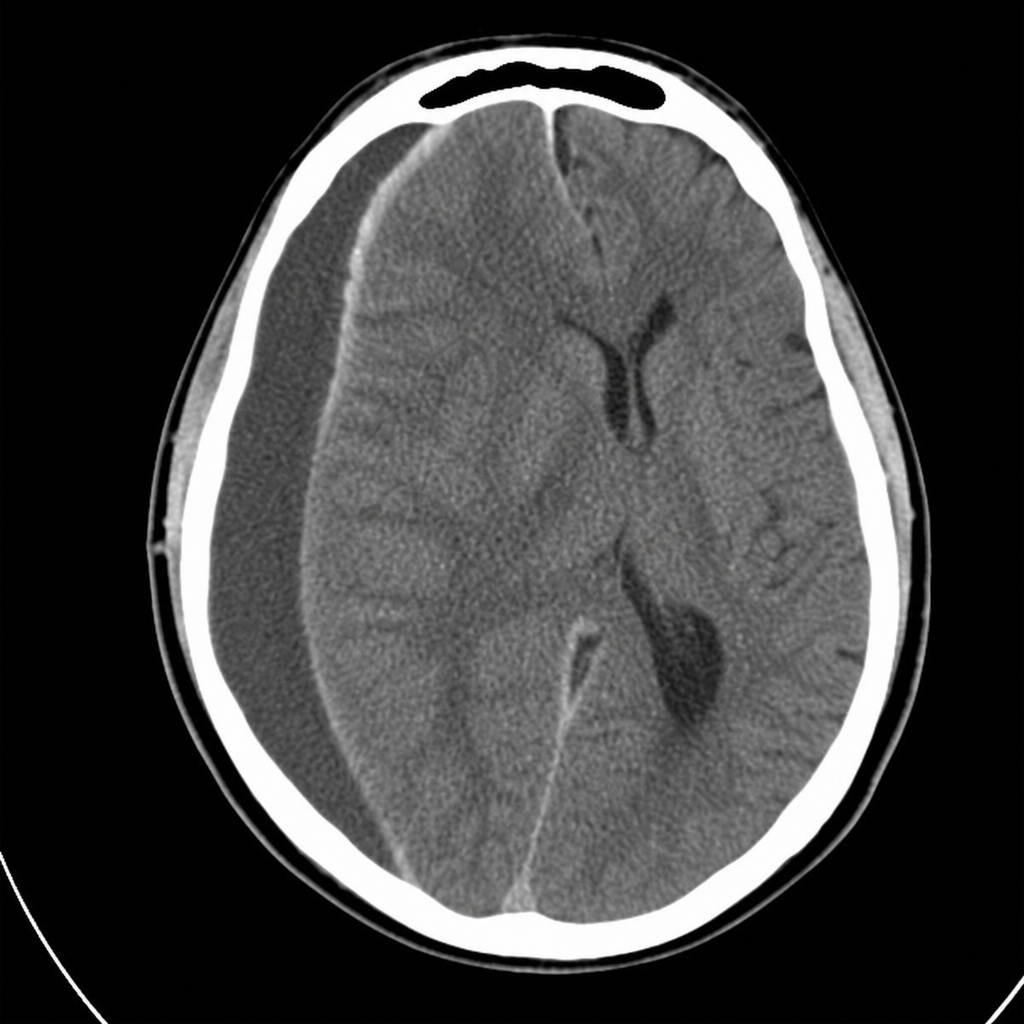
A 27-year-old male is brought to the emergency department with a 1-week history of worsening headache. Over the past 2 days, he has become increasingly confused and developed nausea as well as vomiting. One week ago, he struck his head while exiting a car, but did not lose consciousness. His maternal uncle had a bleeding disorder. He appears in moderate distress. He is oriented to person and time but not to place. His temperature is 37.1°C (98.8°F), pulse is 72/min, respirations are 20/min, and blood pressure is 128/78 mm Hg. Cardiopulmonary examination is unremarkable. His abdomen is soft and nontender. Muscle strength is 5/5 in right upper and right lower extremities, and 3/5 in left upper and left lower extremities. Laboratory studies show: Leukocyte Count 10,000/mm3 Hemoglobin 13.6 g/dL Hematocrit 41% Platelet Count 150,000/mm3 PT 13 seconds aPTT 60 seconds Serum Sodium 140 mEq/L Potassium 4.2 mEq/L Chloride 101 mEq/L Bicarbonate 24 mEq/L Urea Nitrogen 15 mg/dL Creatinine 1.0 mg/dL CT scan of the head is shown. Which of the following is the most likely cause of this patient's symptoms?
A 41-year-old man is admitted to the emergency room after being struck in the abdomen by a large cement plate while transporting it. On initial assessment by paramedics at the scene, his blood pressure was 110/80 mm Hg, heart rate 85/min, with no signs of respiratory distress. On admission, the patient is alert but in distress. He complains of severe, diffuse, abdominal pain and severe weakness. Vital signs are now: blood pressure 90/50 mm Hg, heart rate 96/min, respiratory rate 19/min, temperature 37.4℃ (99.3℉), and oxygen saturation of 95% on room air. His lungs are clear on auscultation. The cardiac exam is significant for a narrow pulse pressure. Abdominal examination reveals a large bruise over the epigastric and periumbilical regions. The abdomen is distended and there is diffuse tenderness to palpation with rebound and guarding, worst in the epigastric region. There is hyperresonance to percussion in the epigastric region and absence of hepatic dullness in the right upper quadrant. Aspiration of the nasogastric tube reveals bloody contents. Focused assessment with sonography for trauma (FAST) shows free fluid in the pelvic region. Evaluation of the perisplenic and perihepatic regions is impossible due to the presence of free air. Aggressive intravenous fluid resuscitation is administered but fails to improve upon the patient’s hemodynamics. Which of the following is the next best step in management?
A 22-year-old soldier sustains a gunshot wound to the left side of the chest during a deployment in Syria. The soldier and her unit take cover from gunfire in a nearby farmhouse, and a combat medic conducts a primary survey of her injuries. She is breathing spontaneously. Two minutes after sustaining the injury, she develops severe respiratory distress. On examination, she is agitated and tachypneic. There is an entrance wound at the midclavicular line at the 2nd rib and an exit wound at the left axillary line at the 4th rib. There is crepitus on the left side of the chest wall. Which of the following is the most appropriate next step in management?
A 62-year-old man comes to the emergency department for severe, acute right leg pain. The patient's symptoms began suddenly 4 hours ago, while he was reading the newspaper. He has poorly-controlled hypertension and osteoarthritis. He has smoked one pack of cigarettes daily for 31 years. Current medications include lisinopril, metoprolol succinate, and ibuprofen. He appears to be in severe pain and is clutching his right leg. His temperature is 37.4°C (99.3°F), pulse is 102/min and irregularly irregular, respirations are 19/min, and blood pressure is 152/94 mm Hg. The right leg is cool to the touch, with decreased femoral, popliteal, posterior tibial, and dorsalis pedis pulses. There is moderate weakness and decreased sensation in the right leg. An ECG shows absent P waves and a variable R-R interval. Right leg Doppler study shows inaudible arterial signal and audible venous signal. Angiography shows 90% occlusion of the right common femoral artery. In addition to initiating heparin therapy, which of the following is the most appropriate next step in management?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app