
Trauma/Emergencies — MCQs

On this page
A 17-year-old boy presents to his primary care physician for eye pain. The patient states that it has been going on for the past 3 days and has been steadily worsening. He recently suffered a superior orbital fracture secondary to playing football without a helmet that required no treatment other than to refrain from contact sports. The patient's past medical history is non-contributory, and his vitals are within normal limits. Physical exam demonstrates pain and swelling inferior to the patient's eye near the lacrimal duct. When pressure is applied to the area expressible pus is noted. Cranial nerves II-XII are grossly intact. Which of the following is the most likely diagnosis?
A 35-year-old man is pulled out of a burning building. He is unconscious and severely injured. He is transported to the nearest emergency department. Upon arrival, he is stabilized and evaluated for burns and trauma. Approximately 40% of his body is covered in burns. The burned areas appear blackened and charred but the skin is mostly intact. It is noted that the patient has loss of pain sensation in the burnt areas with minimal blanching on palpation. The affected area is leathery when palpated. What category of burn did the patient most likely to suffer from?
A 20-year-old woman college volleyball player presents with left shoulder pain and difficulty elevating her left arm. The patient began to experience dull pain in her left shoulder 5 days ago after a volleyball game. The pain is worse when she sleeps with her arm under the pillow or elevates or abducts her left arm. Her temperature is 37.0℃ (98.6℉), the blood pressure is 110/75 mm Hg, the pulse is 66/min, the respiratory rate is 13/min, and the oxygen saturation is 99% on room air. On physical examination, she is alert and cooperative. The left shoulder is normal on the inspection with no swelling or bony deformities. There is point tenderness to palpation of the anterolateral aspect of the left shoulder. Active range of motion of abduction of the left arm is restricted to 70°. Passive range of motion of abduction of the left arm is normal but elicits pain. Strength in the left shoulder is 4/5 and strength in the right shoulder is 5/5. Deep tendon reflexes are 2+ bilaterally. The sensation is intact. Which of the following is the most likely cause of this patient’s condition?
A 15-year-old boy presents to the emergency room with severe lower abdominal pain that awoke him from sleep about 3 hours ago. The pain is sharp and radiates to his left thigh. While in the emergency room, the patient experiences one episode of vomiting. His temperature is 99.3°F (37.4°C), blood pressure is 126/81 mmHg, pulse is 119/min, respirations are 14/min, and oxygen saturation is 99% on room air. Abdominal examination reveals no tenderness in all 4 quadrants. Scrotal examination reveals an elevated left testicle that is diffusely tender. Stroking of the patient's inner thigh on the left side does not result in elevation of the testicle. What is the next step in the management of this patient?
A 45-year-old woman comes to the physician because of right foot pain for 3 months. She has a burning sensation in the plantar area between the third and fourth metatarsals that radiates to the third and fourth digits. She had a right distal radius fracture that was treated with a splint and physical therapy three months ago. She is an account executive and wears high heels to work every day. Vital signs are within normal limits. Examination of the right lower extremity shows intact skin. The posterior tibial and dorsalis pedis pulses are palpable. When pressure is applied to the sole of the foot between the metatarsal heads the patient feels pain and there is an audible click. Tapping on the affected area causes pain that shoots into the third and fourth digits. Which of the following is the most likely diagnosis?
A 54-year-old male carpenter accidentally amputated his right thumb while working in his workshop 30 minutes ago. He reports that he was cutting a piece of wood, and his hand became caught up in the machinery. He is calling the emergency physician for advice on how to transport his thumb and if it is necessary. Which of the following is the best information for this patient?
A 13-year-old boy is brought to the emergency department by his mother because of vomiting and severe testicular pain for 3 hours. The boy has had 4–5 episodes of vomiting during this period. He has never had a similar episode in the past and takes no medications. His father died of testicular cancer at the age of 50. His immunizations are up-to-date. He appears anxious and uncomfortable. His temperature is 37°C (98.6°F), pulse is 90/min, respirations are 14/min, and blood pressure is 100/60 mm Hg. Cardiopulmonary examination shows no abnormalities The abdomen is soft and nondistended. The left scrotum is firm, erythematous, and swollen. There is severe tenderness on palpation of the scrotum that persists on elevation of the testes. Stroking the inner side of the left thigh fails to elicit elevation of the scrotum. Which of the following is the most appropriate next step in management?
A 35-year-old man is brought to the emergency department from a kitchen fire. The patient was cooking when boiling oil splashed on his exposed skin. His temperature is 99.7°F (37.6°C), blood pressure is 127/82 mmHg, pulse is 120/min, respirations are 12/min, and oxygen saturation is 98% on room air. He has dry, nontender, and circumferential burns over his arms bilaterally, burns over the anterior portion of his chest and abdomen, and tender spot burns with blisters on his shins. A 1L bolus of normal saline is administered and the patient is given morphine and his pulse is subsequently 80/min. A Foley catheter is placed which drains 10 mL of urine. What is the best next step in management?
A 17-year-old adolescent male is brought to the emergency department by fire and rescue after being struck by a moving vehicle. The patient reports that he was running through his neighborhood when a car struck him while turning right on a red light. He denies any loss of consciousness. His temperature is 99.0°F (37.2°C), blood pressure is 88/56 mmHg, pulse is 121/min, respirations are 12/min, and SpO2 is 95% on room air. The patient is alert and oriented to person, place and time and is complaining of pain in his abdomen. He has lacerations on his face and extremities. On cardiac exam, he is tachycardic with normal S1 and S2. His lungs are clear to auscultation bilaterally, and his abdomen is soft but diffusely tender to palpation. The patient tenses his abdomen when an abdominal exam is performed. Bowel sounds are present, and he is moving all 4 extremities spontaneously. His skin is cool with delayed capillary refill. After the primary survey, 2 large-bore IVs are placed, and the patient is given a bolus of 2 liters of normal saline. Which of the following is the best next step in management?
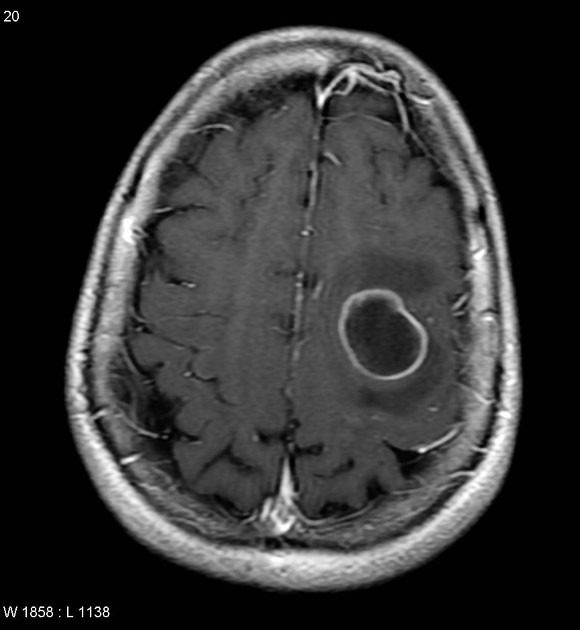
A 42-year-old man is brought to the physician 25 minutes after an episode of violent jerky movements of his hands and legs that lasted for 5 minutes. After the episode, he had difficulty conversing. For the past 10 days, he has had a left-sided headache and nausea. Apart from a history of recurrent ear infections treated with antibiotics, he reports no other personal or family history of serious illness. He works as an assistant at a veterinarian clinic. He appears ill and is oriented to place and person only. His temperature is 37.8°C (100°F), pulse is 102/min, and blood pressure 112/78 mm Hg. Examination shows bilateral optic disc swelling. There is no lymphadenopathy. Muscle strength and tone is normal in all extremities. Deep tendon reflexes are 2+ bilaterally. Plantar reflex shows a flexor response bilaterally. Laboratory studies show a CD4 count within the reference range. An MRI of the brain is shown. Intravenous mannitol and levetiracetam are administered. Which of the following is the most appropriate next step in management?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app