
Trauma/Emergencies — MCQs

On this page
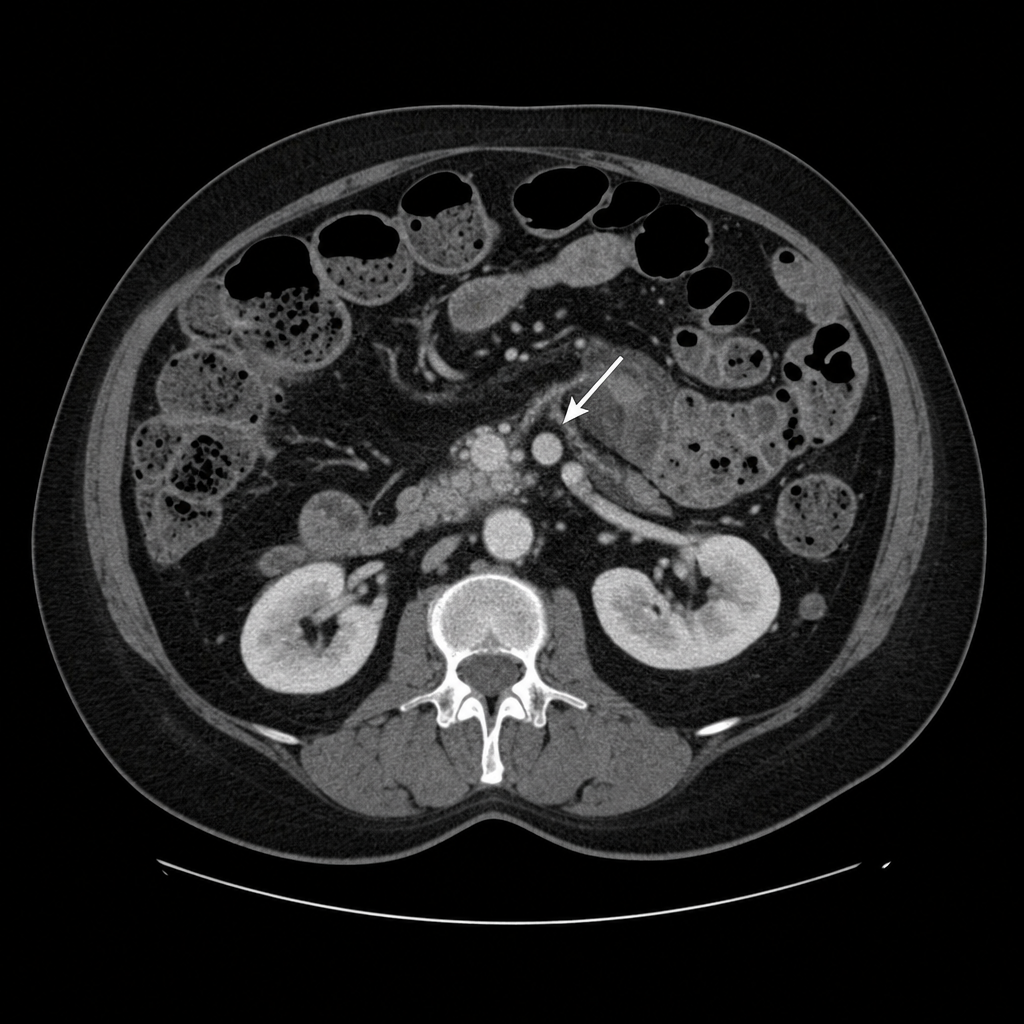
A 67-year-old woman with a history of atrial fibrillation on warfarin presents with sudden-onset severe periumbilical pain that is disproportionate to her abdominal tenderness on examination. She has nausea and one episode of vomiting. Vital signs: BP 110/72 mmHg, HR 108 bpm, RR 18/min, temperature 37.2°C. Abdominal examination reveals mild diffuse tenderness without rigidity or guarding. Bowel sounds are present. INR is 3.1. CT abdomen with contrast demonstrates occlusion of the superior mesenteric artery with segmental bowel wall thickening and pneumatosis intestinalis, consistent with established bowel infarction. Which of the following is the most appropriate next step in management?
A 30-year-old male gang member is brought to the emergency room with a gunshot wound to the abdomen. The patient was intubated and taken for an exploratory laparotomy, which found peritoneal hemorrhage and injury to the small bowel. He required 5 units of blood during this procedure. Following the operation, the patient was sedated and remained on a ventilator in the surgical intensive care unit (SICU). The next day, a central line is placed and the patient is started on total parenteral nutrition. Which of the following complications is most likely in this patient?
A 45-year-old man is brought to the trauma bay by emergency services after a motorbike accident in which the patient, who was not wearing a helmet, hit a pole of a streetlight with his head. When initially evaluated by the paramedics, the patient was responsive, albeit confused, opened his eyes spontaneously, and was able to follow commands. An hour later, upon admission, the patient only opened his eyes to painful stimuli, made incomprehensible sounds, and assumed a flexed posture. The vital signs are as follows: blood pressure 140/80 mm Hg; heart rate 59/min; respiratory rate 11/min; temperature 37.0℃ (99.1℉), and SaO2, 95% on room air. The examination shows a laceration and bruising on the left side of the head. There is anisocoria with the left pupil 3 mm more dilated than the right. Both pupils react sluggishly to light. There is an increase in tone and hyperreflexia in the right upper and lower extremities. The patient is intubated and mechanically ventilated, head elevated to 30°, and sent for a CT scan. Which of the following management strategies should be used in this patient, considering his most probable diagnosis?
An 18-year-old man presents to the emergency department with complaints of sudden severe groin pain and swelling of his left testicle. It started roughly 5 hours ago and has been progressively worsening. History reveals that he has had multiple sexual partners but uses condoms regularly. Vital signs include: blood pressure 120/80 mm Hg, heart rate 84/min, respiratory rate 18/min, and temperature 36.6°C (98.0°F). Physical examination reveals that he has an impaired gait and a tender, horizontal, high-riding left testicle and absent cremasteric reflex. Which of the following is the best next step for this patient?
A 63-year-old female with known breast cancer presents with progressive motor weakness in bilateral lower extremities and difficulty ambulating. Physical exam shows 4 of 5 motor strength in her legs and hyper-reflexia in her patellar tendons. Neurologic examination 2 weeks prior was normal. Imaging studies, including an MRI, show significant spinal cord compression by the metastatic lesion and complete erosion of the T12 vertebrae. She has no metastatic disease to the visceral organs and her oncologist reports her life expectancy to be greater than one year. What is the most appropriate treatment?
A 25-year-old man is brought to the emergency department because of a 6-day history of fever and chills. During this period, he has had generalized weakness, chest pain, and night sweats. He has a bicuspid aortic valve and recurrent migraine attacks. He has smoked one pack of cigarettes daily for 5 years. He does not drink alcohol. He has experimented with intravenous drugs in the past but has not used any illicit drugs in the last two months. Current medications include propranolol and a multivitamin. He appears ill. His temperature is 39°C (102.2°F), pulse is 108/min, respirations are 14/min, and blood pressure is 150/50 mm Hg. Diffuse crackles are heard. A grade 3/6 high-pitched, early diastolic, decrescendo murmur is best heard along the left sternal border. An S3 gallop is heard. The remainder of the physical examination shows no abnormalities. Laboratory studies show: Hemoglobin 13.1 g/dL Leukocyte count 13,300/mm3 Platelet count 270,000/mm3 Serum Glucose 92 mg/dL Creatinine 0.9 mg/dL Total bilirubin 0.4 mg/dL AST 25 U/L ALT 28 U/L Three sets of blood cultures are sent to the laboratory. Transthoracic echocardiography confirms the diagnosis. In addition to antibiotic therapy, which of the following is the most appropriate next step in management?
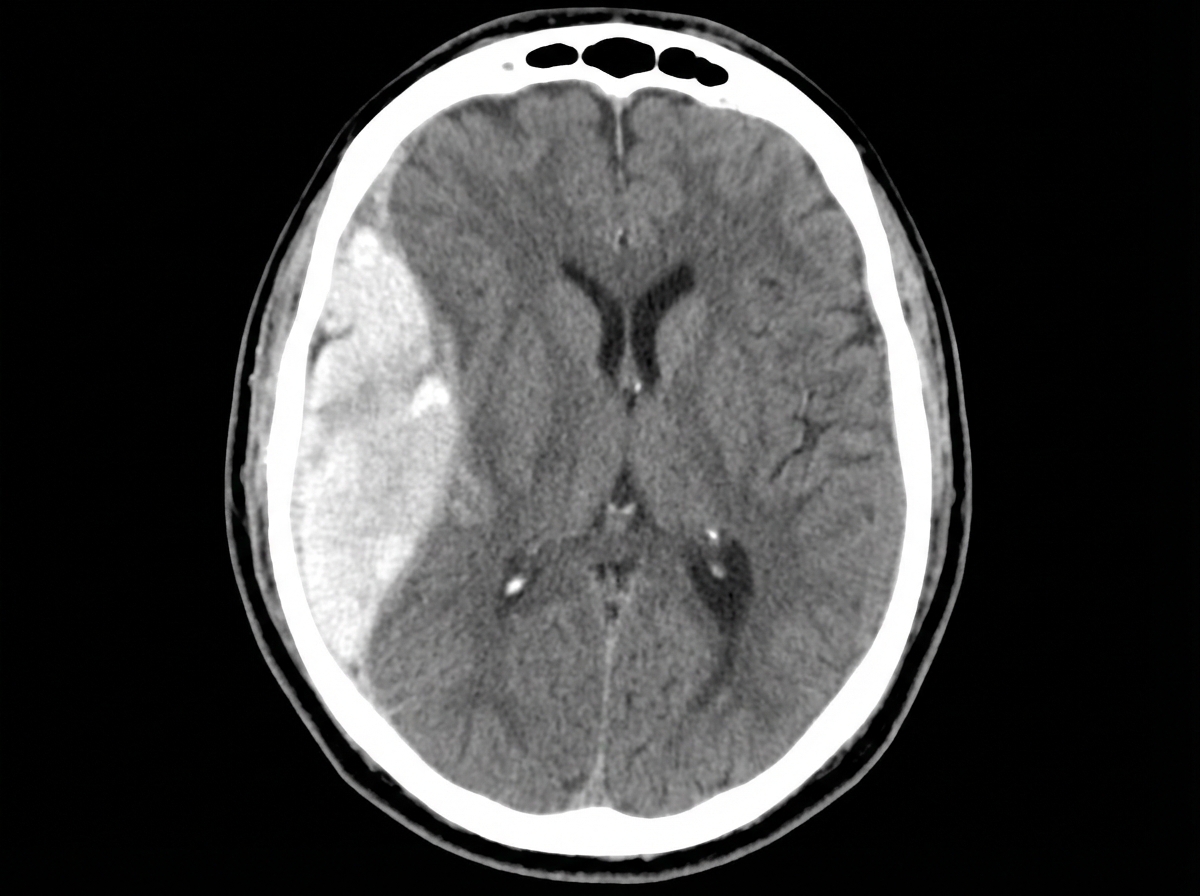
A 47-year-old man is admitted to the emergency room after a fight in which he was hit in the head with a hammer. The witnesses say that the patient initially lost consciousness, but regained consciousness by the time emergency services arrived. On admission, the patient complained of a diffuse headache. He opened his eyes spontaneously, was verbally responsive, albeit confused, and was able to follow commands. He could not elevate his left hand and leg. He did not remember the events prior to the loss of consciousness and had difficulty remembering information, such as the names of nurses or doctors. His airway was not compromised. The vital signs are as follows: blood pressure, 180/100 mm Hg; heart rate, 59/min; respiratory rate, 12/min; temperature 37.0℃ (98.6℉); and SaO2, 96% on room air. The examination revealed bruising in the right frontotemporal region. The pupils are round, equal, and show a poor response to light. The neurologic examination shows hyperreflexia and decreased power in the left upper and lower limbs. There is questionable nuchal rigidity, but no Kernig and Brudzinski signs. The CT scan is shown in the image. Which of the following options is recommended for this patient?
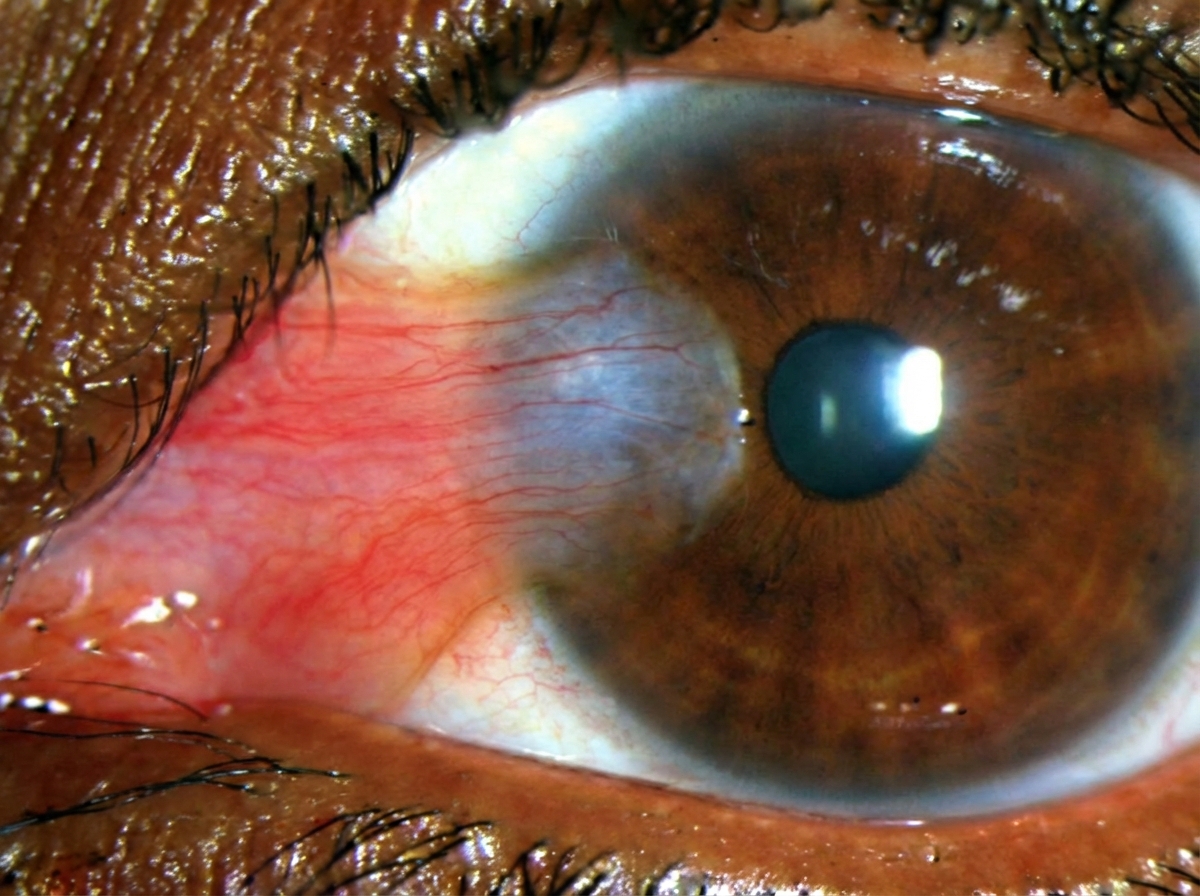
A 65-year-old man is brought to his primary care provider by his concerned wife. She reports he has had this "thing" on his eye for years and refuses to seek care. He denies any pain or discharge from the affected eye. A picture of his eye is shown below. Given the diagnosis, what are you most likely to discover when taking this patient's history?
A 31-year-old woman is brought to the emergency department 25 minutes after sustaining a gunshot wound to the neck. She did not lose consciousness. On arrival, she has severe neck pain. She appears anxious. Her temperature is 37°C (98.6°F), pulse is 105/min, respirations are 25/min, and blood pressure is 100/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. She is oriented to person, place, and time. Examination shows a bullet entrance wound in the right posterior cervical region of the neck. There is no exit wound. Carotid pulses are palpable bilaterally. There are no carotid bruits. Sensation to pinprick and light touch is normal. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. In addition to intravenous fluid resuscitation, which of the following is the most appropriate next step in the management of this patient?
A 41-year-old man is brought to the emergency department 3 hours after falling while mountain biking and hitting his head. Initially, he refused treatment, but an hour ago he began to develop a severe headache, nausea, and left leg weakness. He has no visual changes and is oriented to person, time, and place. His temperature is 37°C (98.6°F), pulse is 68/min, respirations are 17/min and regular, and blood pressure is 130/78 mm Hg. Examination shows a 5-cm bruise on the right side of his skull. The pupils are equal, round, and reactive to light and accommodation. Muscle strength is 0/5 in his left knee and foot. Which of the following is the most likely cause of this patient's presentation?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app