
Rejection diagnosis and management — MCQs

A 55-year-old woman recently underwent kidney transplantation for end-stage renal disease. Her early postoperative period was uneventful, and her serum creatinine is lowered from 4.3 mg/dL (preoperative) to 2.5 mg/dL. She is immediately started on immunosuppressive therapy. On postoperative day 7, she presents to the emergency department (ED) because of nausea, fever, abdominal pain at the transplant site, malaise, and pedal edema. The vital signs include: pulse 106/min, blood pressure 167/96 mm Hg, respirations 26/min, and temperature 40.0°C (104.0°F). The surgical site shows no signs of infection. Her urine output is 250 mL over the past 24 hours. Laboratory studies show: Hematocrit 33% White blood cell (WBC) count 6700/mm3 Blood urea 44 mg/dL Serum creatinine 3.3 mg/dL Serum sodium 136 mEq/L Serum potassium 5.6 mEq/L An ultrasound of the abdomen shows collection of fluid around the transplanted kidney with moderate hydronephrosis. Which of the following initial actions is the most appropriate?
A 10-year-old boy is presented to the hospital for a kidney transplant. In the operating room, the surgeon connects an allograft kidney renal artery to the aorta, and after a few moments, the kidney becomes cyanotic, edematous, and dusky with mottling. Which of the following in the recipient’s serum is responsible for this rejection?
A 62-year-old female with a history of uncontrolled hypertension undergoes kidney transplantation. One month following surgery she has elevated serum blood urea nitrogen and creatinine and the patient complains of fever and arthralgia. Her medications include tacrolimus and prednisone. If the patient were experiencing acute, cell-mediated rejection, which of the following would you most expect to see upon biopsy of the transplanted kidney?
A 61-year-old-male underwent deceased donor liver transplantation 3 weeks ago. During his follow up visit he complains of nausea and abdominal pain. He has been taking all of his medications as prescribed. He has a history of alcohol abuse and his last drink was one year ago. He does not smoke cigarettes and lives at home with his wife. On physical examination temperature is 98.6°F (37°C), blood pressure is 115/80 mmHg, pulse is 90/min, respirations are 18/min, and pulse oximetry is 99% on room air. He has scleral icterus and a positive fluid wave. Liver function tests are as follows: Alkaline phosphatase: 110 U/L Aspartate aminotransferase (AST, GOT): 100 U/L Alanine aminotransferase (ALT, GPT): 120 U/L Bilirubin total: 2.2 mg/dL Liver biopsy shows mixed dense interstitial lymphocytic infiltrates in the portal triad. What is the mechanism of this reaction?
A 57-year-old woman comes to the clinic complaining of decreased urine output. She reports that over the past 2 weeks she has been urinating less and less every day. She denies changes in her diet or fluid intake. The patient has a history of lupus nephritis, which has resulted in end stage renal disease. She underwent a renal transplant 2 months ago. Since then she has been on mycophenolate and cyclosporine, which she takes as prescribed. The patient’s temperature is 99°F (37.2°C), blood pressure is 172/102 mmHg, pulse is 88/min, and respirations are 17/min with an oxygen saturation of 97% on room air. Labs show an elevation in serum creatinine and blood urea nitrogen. On physical examination, she has 2+ pitting edema of the bilateral lower extremities. Lungs are clear to auscultation. Urinalysis shows elevated protein. A post-void bladder scan is normal. A renal biopsy is obtained, which shows lymphocyte infiltration and intimal swelling. Which of the following is the next best step in management?
An investigator studying immune-mediated pulmonary damage performs an autopsy on a bilateral lung transplant recipient who died of hypercapnic respiratory failure. The patient underwent lung transplantation for idiopathic pulmonary fibrosis. Microscopic examination of the lung shows diffuse eosinophilic scarring of the terminal and respiratory bronchioles and near-complete luminal obliteration by polypoidal plugs of granulation tissue. Examination of the skin shows no abnormalities. The findings in this patient are most consistent with which of the following conditions?
Several weeks following a kidney transplantation, a 50-year-old Caucasian female presents for evaluation of the transplanted organ. Biopsy shows inflammation involving the endothelial cells of the kidney vasculature and the presence of mononuclear cells in the interstitium. Which cells are most likely responsible for this presentation?
A 14-year-old boy has undergone kidney transplantation due to stage V chronic kidney disease. A pre-transplantation serologic assessment showed that he is negative for past or present HIV infection, viral hepatitis, EBV, and CMV infection. He has a known allergy for macrolides. The patient has no complaints 1 day after transplantation. His vital signs include: blood pressure 120/70 mm Hg, heart rate 89/min, respiratory rate 17/min, and temperature 37.0°C (98.6°F). On physical examination, the patient appears to be pale, his lungs are clear on auscultation, heart sounds are normal, and his abdomen is non-tender on palpation. His creatinine is 0.65 mg/dL (57.5 µmol/L), GFR is 71.3 mL/min/1.73 m2, and urine output is 0.9 mL/kg/h. Which of the following drugs should be used in the immunosuppressive regimen in this patient?
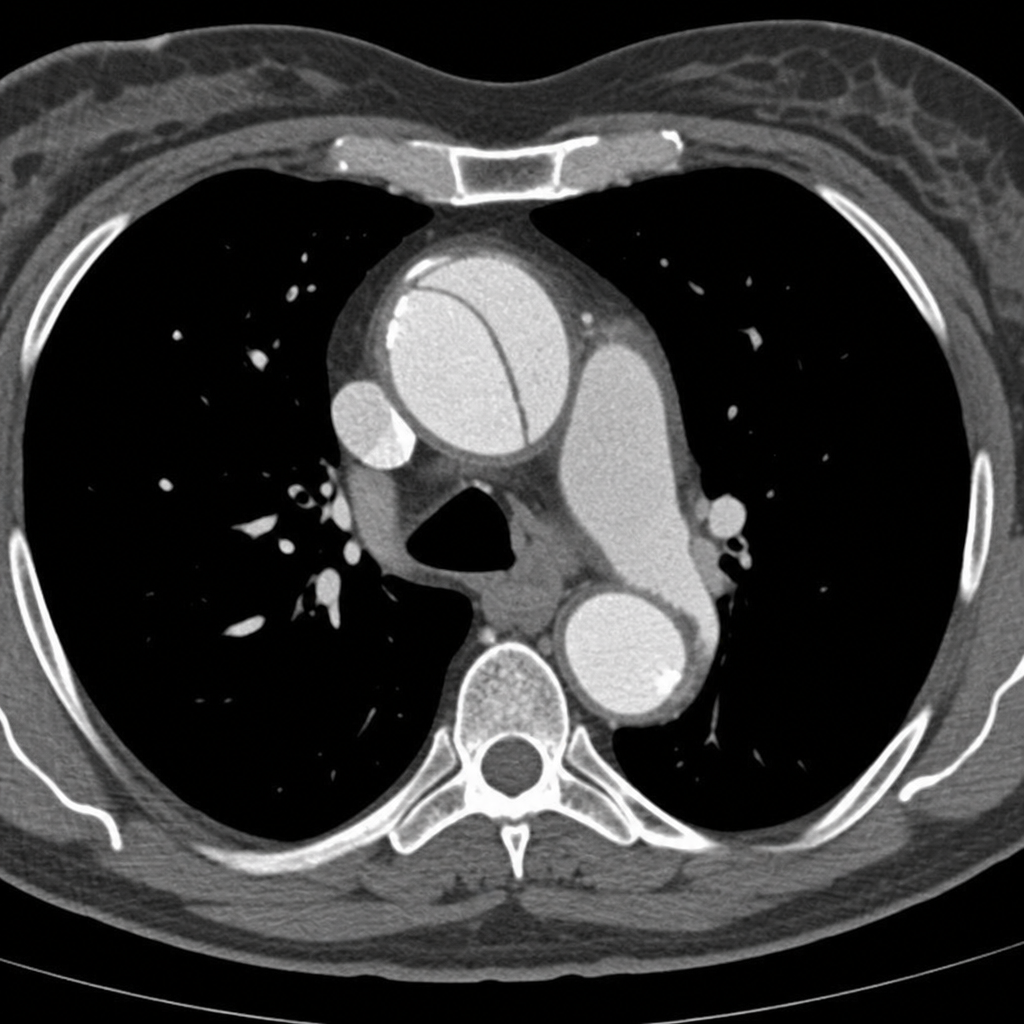
A 45-year-old woman presents to the emergency department with sudden-onset severe tearing chest pain radiating to the interscapular region. Her blood pressure is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. She is diaphoretic and in moderate distress. A CT angiogram of the chest is obtained and demonstrates an intimal flap involving the ascending aorta, consistent with a Stanford Type A aortic dissection. Based on the imaging findings, which of the following is the most appropriate next step in management?
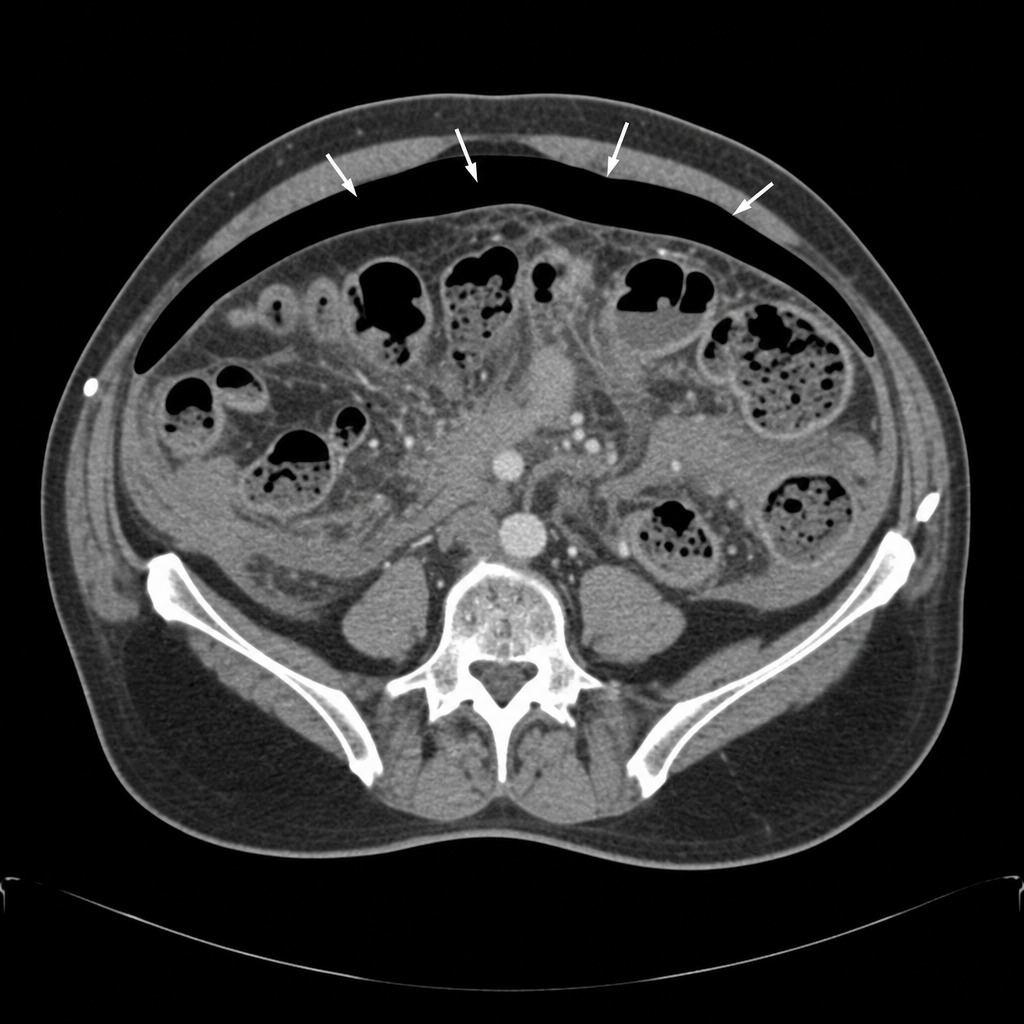
A 58-year-old woman undergoes an elective sigmoid colectomy for recurrent diverticulitis. On postoperative day 6, she develops a temperature of 38.9°C, HR of 118 bpm, and BP of 88/54 mmHg despite 2L of IV fluid resuscitation. She complains of worsening lower abdominal pain. Her abdomen is diffusely tender with guarding and rigidity. WBC is 19,500/µL. A CT scan of the abdomen and pelvis with contrast demonstrates free intraperitoneal air and diffuse pelvic fluid consistent with an uncontained anastomotic leak. Based on the CT findings, what is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app