
Long-term complications of transplantation — MCQs

Two weeks after undergoing allogeneic stem cell transplant for multiple myeloma, a 55-year-old man develops a severely pruritic rash, abdominal cramps, and profuse diarrhea. He appears lethargic. Physical examination shows yellow sclerae. There is a generalized maculopapular rash on his face, trunk, and lower extremities, and desquamation of both soles. His serum alanine aminotransferase is 115 U/L, serum aspartate aminotransferase is 97 U/L, and serum total bilirubin is 2.7 mg/dL. Which of the following is the most likely underlying cause of this patient's condition?
A 31-year-old female receives a kidney transplant for autosomal dominant polycystic kidney disease (ADPKD). Three weeks later, the patient experiences acute, T-cell mediated rejection of the allograft and is given sirolimus. Which of the following are side effects of this medication?
Twelve days after undergoing a cadaveric renal transplant for adult polycystic kidney disease, a 23-year-old man has pain in the right lower abdomen and generalized fatigue. During the past 4 days, he has had decreasing urinary output. Creatinine concentration was 2.3 mg/dL on the second postoperative day. Current medications include prednisone, cyclosporine, azathioprine, and enalapril. His temperature is 38°C (100.4°F), pulse is 103/min, and blood pressure is 168/98 mm Hg. Examination reveals tenderness to palpation on the graft site. Creatinine concentration is 4.3 mg/dL. A biopsy of the transplanted kidney shows tubulitis. C4d staining is negative. Which of the following is the most likely cause of this patient's findings?
A 57-year-old woman comes to the clinic complaining of decreased urine output. She reports that over the past 2 weeks she has been urinating less and less every day. She denies changes in her diet or fluid intake. The patient has a history of lupus nephritis, which has resulted in end stage renal disease. She underwent a renal transplant 2 months ago. Since then she has been on mycophenolate and cyclosporine, which she takes as prescribed. The patient’s temperature is 99°F (37.2°C), blood pressure is 172/102 mmHg, pulse is 88/min, and respirations are 17/min with an oxygen saturation of 97% on room air. Labs show an elevation in serum creatinine and blood urea nitrogen. On physical examination, she has 2+ pitting edema of the bilateral lower extremities. Lungs are clear to auscultation. Urinalysis shows elevated protein. A post-void bladder scan is normal. A renal biopsy is obtained, which shows lymphocyte infiltration and intimal swelling. Which of the following is the next best step in management?
A 46-year-old man comes to the physician because of a 4-month history of progressively worsening fatigue and loss of appetite. Five years ago, he received a kidney transplant from a living family member. Current medications include sirolimus and mycophenolate. His blood pressure is 150/95 mm Hg. Laboratory studies show normocytic, normochromic anemia and a serum creatinine concentration of 3.1 mg/dL; his vital signs and laboratory studies were normal 6 months ago. Which of the following is the most likely underlying mechanism of this patient’s increase in creatinine concentration?
Several weeks following a kidney transplantation, a 50-year-old Caucasian female presents for evaluation of the transplanted organ. Biopsy shows inflammation involving the endothelial cells of the kidney vasculature and the presence of mononuclear cells in the interstitium. Which cells are most likely responsible for this presentation?
A 50-year-old woman comes to the physician for the evaluation of excessive hair growth on her chin over the past 2 weeks. She also reports progressive enlargement of her gums. Three months ago, she underwent a liver transplantation due to Wilson disease. Following the procedure, the patient was started on transplant rejection prophylaxis. She has a history of poorly-controlled type 2 diabetes mellitus. Temperature is 37°C (98.6°F), pulse is 80/min, respirations are 22/min, and blood pressure is 150/80 mm Hg. Physical examination shows dark-pigmented, coarse hair on the chin, upper lip, and chest. The gingiva and the labial mucosa are swollen. There is a well-healed scar on her right lower abdomen. Which of the following drugs is the most likely cause of this patient's findings?
Fourteen days after a laparoscopic cholecystectomy for cholelithiasis, a 45-year-old woman comes to the emergency department because of persistent episodic epigastric pain for 3 days. The pain radiates to her back, occurs randomly throughout the day, and is associated with nausea and vomiting. Each episode lasts 30 minutes to one hour. Antacids do not improve her symptoms. She has hypertension and fibromyalgia. She has smoked 1–2 packs of cigarettes daily for the past 10 years and drinks 4 cans of beer every week. She takes lisinopril and pregabalin. She appears uncomfortable. Her temperature is 37°C (98.6° F), pulse is 84/min, respirations are 14/min, and blood pressure is 127/85 mm Hg. Abdominal examination shows tenderness to palpation in the upper quadrants without rebound or guarding. Bowel sounds are normal. The incisions are clean, dry, and intact. Serum studies show: AST 80 U/L ALT 95 U/L Alkaline phosphatase 213 U/L Bilirubin, total 1.3 mg/dL Direct 0.7 mg/dL Amylase 52 U/L Abdominal ultrasonography shows dilation of the common bile duct and no gallstones. Which of the following is the most appropriate next step in management?
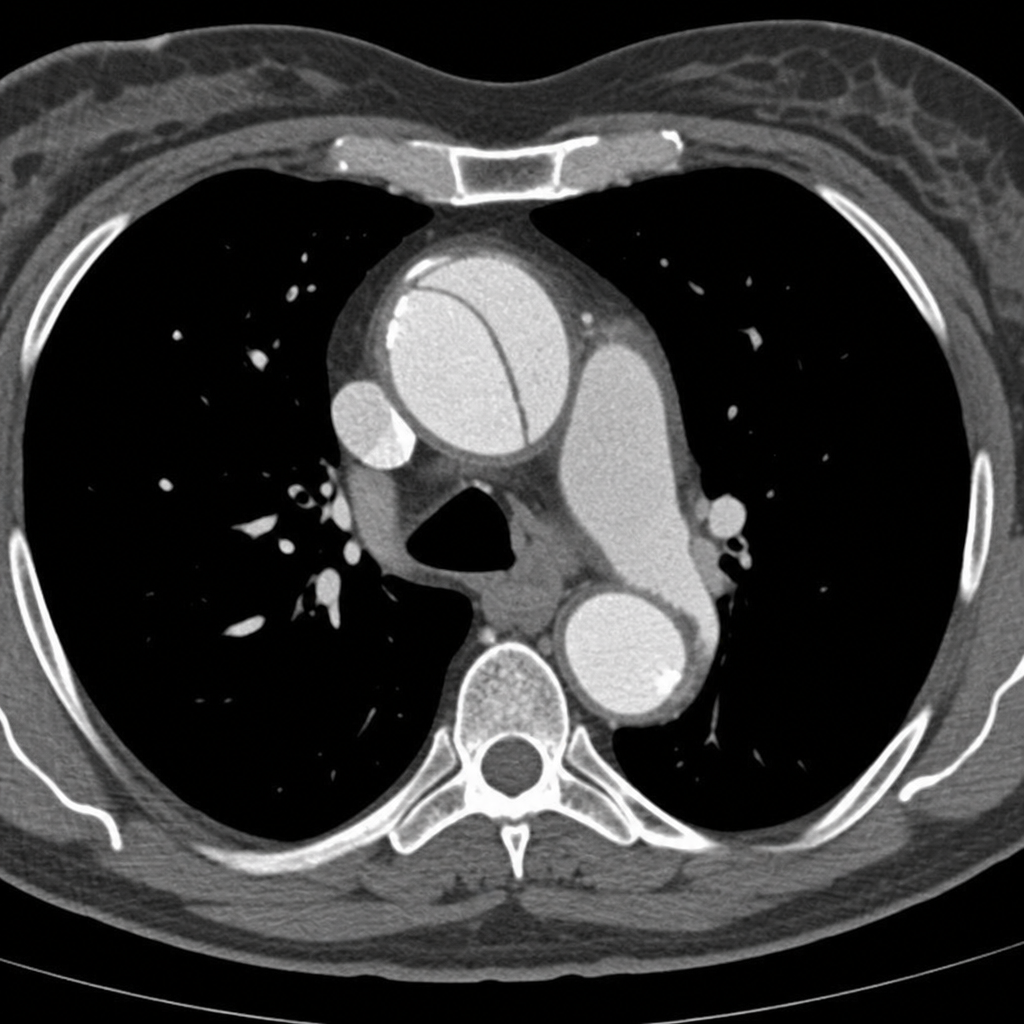
A 45-year-old woman presents to the emergency department with sudden-onset severe tearing chest pain radiating to the interscapular region. Her blood pressure is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. She is diaphoretic and in moderate distress. A CT angiogram of the chest is obtained and demonstrates an intimal flap involving the ascending aorta, consistent with a Stanford Type A aortic dissection. Based on the imaging findings, which of the following is the most appropriate next step in management?
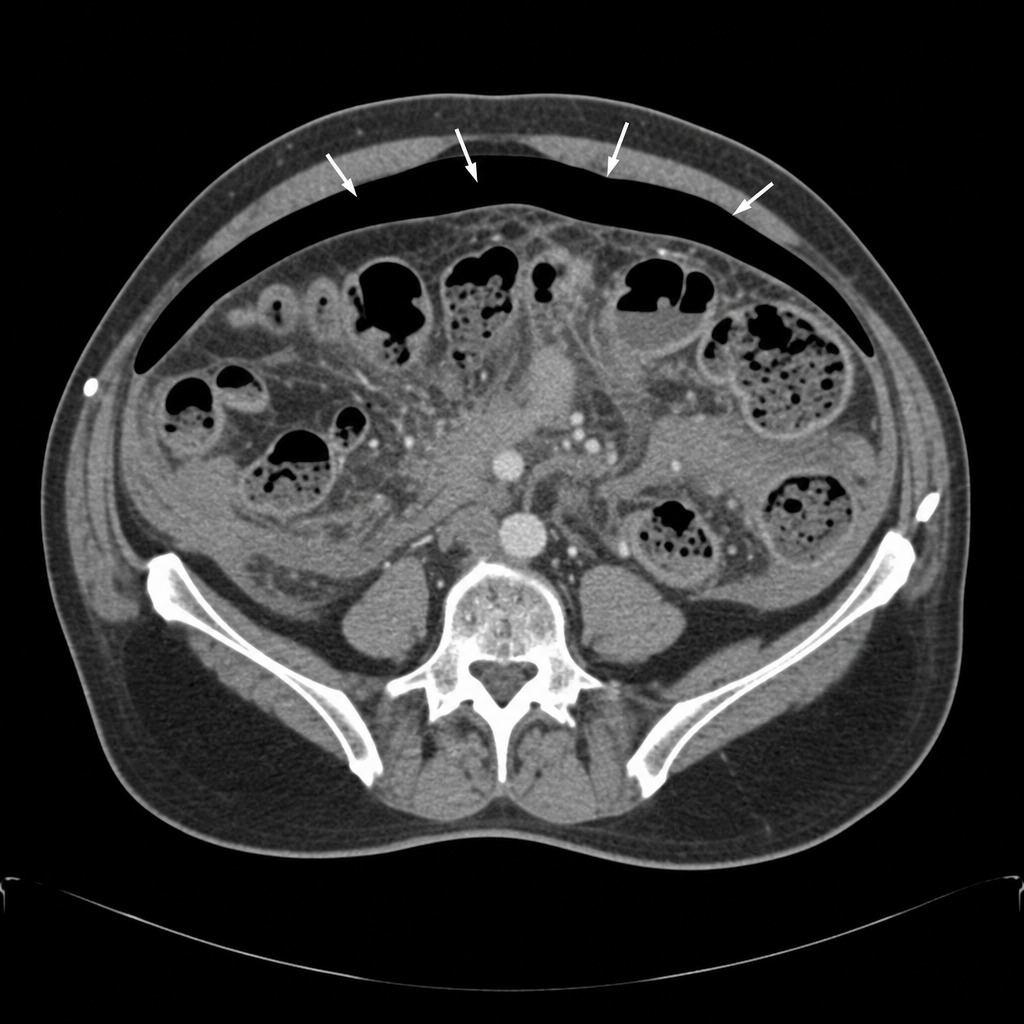
A 58-year-old woman undergoes an elective sigmoid colectomy for recurrent diverticulitis. On postoperative day 6, she develops a temperature of 38.9°C, HR of 118 bpm, and BP of 88/54 mmHg despite 2L of IV fluid resuscitation. She complains of worsening lower abdominal pain. Her abdomen is diffusely tender with guarding and rigidity. WBC is 19,500/µL. A CT scan of the abdomen and pelvis with contrast demonstrates free intraperitoneal air and diffuse pelvic fluid consistent with an uncontained anastomotic leak. Based on the CT findings, what is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app