
Liver transplantation — MCQs

A 60-year-old rock musician presents to the office because he has been feeling increasingly tired for the past 6 months. He has a history of intravenous drug use and alcohol abuse. He states that he feels quite tired, but he otherwise has no complaints. Physical examination is noncontributory. His laboratory values are normal other than moderately elevated liver enzymes. Which of the following additional tests should you order first?
A 22-year-old man is brought to the emergency department by ambulance 1 hour after a motor vehicle accident. He did not require any circulatory resuscitation at the scene, but he was intubated because he was unresponsive. He has no history of serious illnesses. He is on mechanical ventilation with no sedation. His blood pressure is 121/62 mm Hg, the pulse is 68/min, and the temperature is 36.5°C (97.7°F). His Glasgow coma scale (GCS) is 3. Early laboratory studies show no abnormalities. A search of the state donor registry shows that he has registered as an organ donor. Which of the following is the most appropriate next step in evaluation?
A patient with HCC and a long history of alcohol dependence and chronic hepatitis C has been using the mTOR inhibitor sirolimus 100 mg for cancer treatment. Her cancer has shown a partial response. She also has a history of hypertension and poorly controlled type 2 diabetes mellitus complicated by diabetic retinopathy. Current medications include enalapril and insulin. She asks her oncologist and hepatologist if she could try everolimus for its purported survival benefit in treating HCC. Based on clinical considerations, which of the following statements is most accurate?
A 56-year-old woman is brought to the emergency department by her family with altered mental status. Her husband says that she complained of fever, vomiting, and abdominal pain 2 days ago. She has a history of long-standing alcoholism and previous episodes of hepatic encephalopathy. Current vital signs include a temperature of 38.3°C (101°F), blood pressure of 85/60 mm Hg, pulse of 95/min, and a respiratory rate 30/min. On physical examination, the patient appears ill and obtunded. She is noted to have jaundice, a palpable firm liver, and massive abdominal distension with shifting dullness. Which of the following is the best initial step in management of this patient's condition?
A 67-year-old man is seen on the surgical floor after a transplant procedure. The previous day, the patient had a renal transplant from a matched donor. He is currently recovering and doing well. The patient has a past medical history of IV drug use, diabetes mellitus, oral cold sores, hypertension, renal failure, and dyslipidemia. The patient's current medications include lisinopril, atorvastatin, insulin, and aspirin. Prior to the procedure, he was also on dialysis. The patient is started on cyclosporine. The patient successfully recovers over the next few days. Which of the following medications should be started in this patient?
An epidemiologist is evaluating the efficacy of Noxbinle in preventing HCC deaths at the population level. A clinical trial shows that over 5 years, the mortality rate from HCC was 25% in the control group and 15% in patients treated with Noxbinle 100 mg daily. Based on this data, how many patients need to be treated with Noxbinle 100 mg to prevent, on average, one death from HCC?
A 57-year-old man presents to the emergency department with fatigue. He states that his symptoms started yesterday and have been worsening steadily. The patient endorses a recent weight loss of 7 pounds this past week and states that he feels diffusely itchy. The patient has a past medical history of alcohol abuse, obesity, asthma, and IV drug use. His current medications include metformin, atorvastatin, albuterol, and fluticasone. In addition, the patient admits to smoking and drinking more than usual lately due to the stress he has experienced. His temperature is 98.7°F (37.1°C), blood pressure is 130/75 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam is notable for an ill-appearing man. The patient's skin appears yellow. Abdominal exam is notable for right upper quadrant tenderness. Cardiac and pulmonary exams are within normal limits. Laboratory values are ordered as seen below: Hemoglobin: 14 g/dL Hematocrit: 42% Leukocyte count: 5,500 cells/mm^3 with normal differential Platelet count: 70,000/mm^3 Partial thromboplastin time: 92 seconds Prothrombin time: 42 seconds AST: 1110 U/L ALT: 990 U/L Which of the following is most likely to be found in this patient's history?
A 58-year-old man is brought to the emergency department because of confusion, weight loss, and anuria. He has chronic kidney disease, hypertension, and type 2 diabetes mellitus. He was diagnosed with acute lymphoblastic leukemia at the age of 8 years and was treated with an allogeneic stem cell transplantation. He is HIV-positive and has active hepatitis C virus infection. He drinks around 8 cans of beer every week. His current medications include tenofovir, emtricitabine, atazanavir, daclatasvir, sofosbuvir, insulin, amlodipine, and enalapril. He appears lethargic. His temperature is 36°C (96.8°F), pulse is 130/min, respirations are 26/min, and blood pressure is 145/90 mm Hg. Examination shows severe edema in his legs and generalized muscular weakness. Auscultation of the lung shows crepitant rales. Laboratory studies show positive HCV antibody and positive HCV RNA. His HIV viral load is undetectable and his CD4+ T-lymphocyte count is 589/μL. Six months ago, his CD4+ T-lymphocyte count was 618/μL. An ECG of the heart shows arrhythmia with frequent premature ventricular contractions. Arterial blood gas analysis on room air shows: pH 7.23 PCO2 31 mm Hg HCO3- 13 mEq/L Base excess -12 mEq/L The patient states he would like to donate organs or tissues in the case of his death. Which of the following is an absolute contraindication for organ donation in this patient?
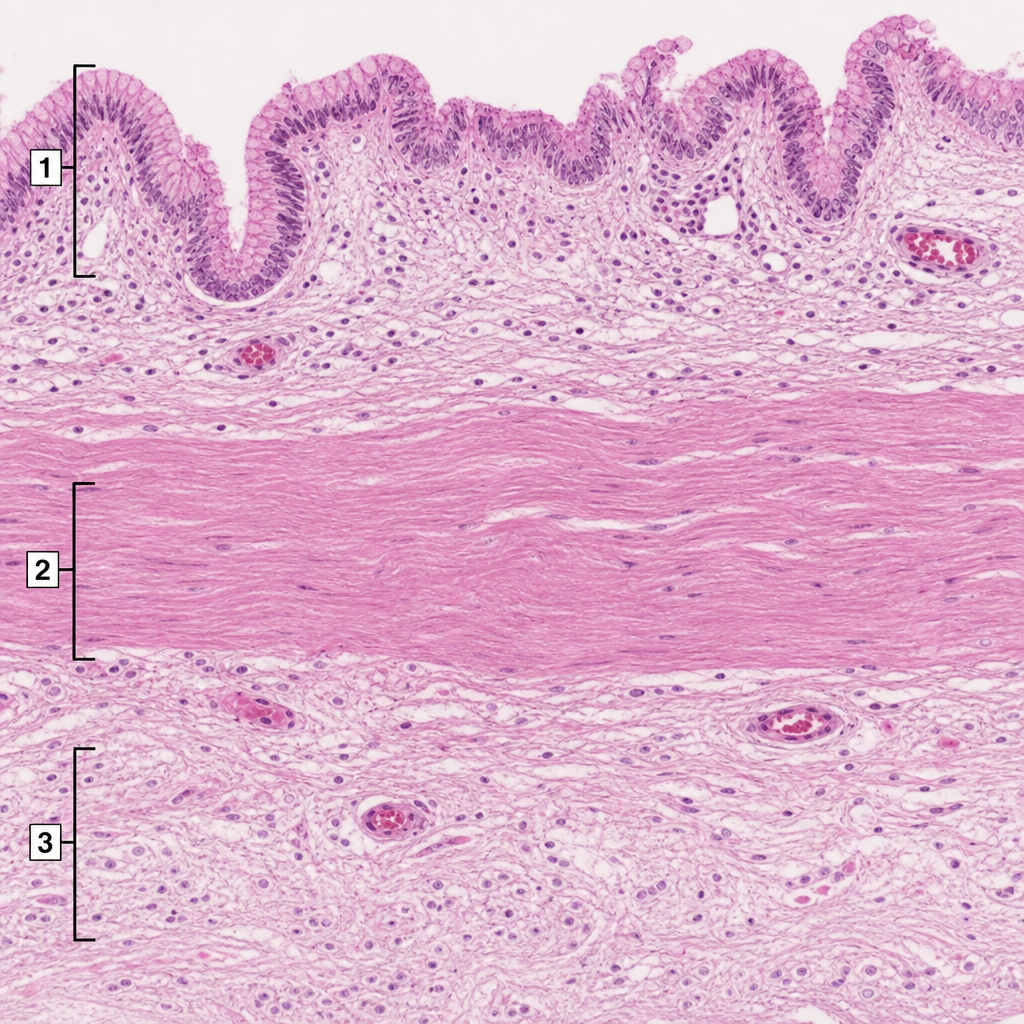
A 36-year-old man undergoes surgical intervention due to a right upper quadrant stab wound. His gallbladder was found to be lacerated and is removed. It is sent for histological evaluation. The pathologist examines the slide shown in the exhibit and identifies several structures numbered the image. Which of the following statements is correct?
A 37-year-old man who had undergone liver transplantation 7 years ago, presents to the physician because of yellowish discoloration of the skin, sclera, and urine. He is on regular immunosuppressive therapy and is well-adherent to the treatment. He has no comorbidities and is not taking any other medication. He provides a history of similar episodes of yellowish skin discoloration 6–7 times since he underwent liver transplantation. Physical examination shows clinical jaundice. Laboratory studies show: While blood cell (WBC) count 4,400/mm3 Hemoglobin 11.1 g/dL Serum creatinine 0.9 mg/dL Serum bilirubin (total) 44 mg/dL Aspartate transaminase (AST) 1,111 U/L Alanine transaminase (ALT) 671 U/L Serum gamma-glutamyl transpeptidase 777 U/L Alkaline phosphatase 888 U/L Prothrombin time 17 seconds A Doppler ultrasound shows significantly reduced blood flow into the transplanted liver. A biopsy of the transplanted liver is likely to show which of the following histological features?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app