
Transplant medicine — MCQs

On this page
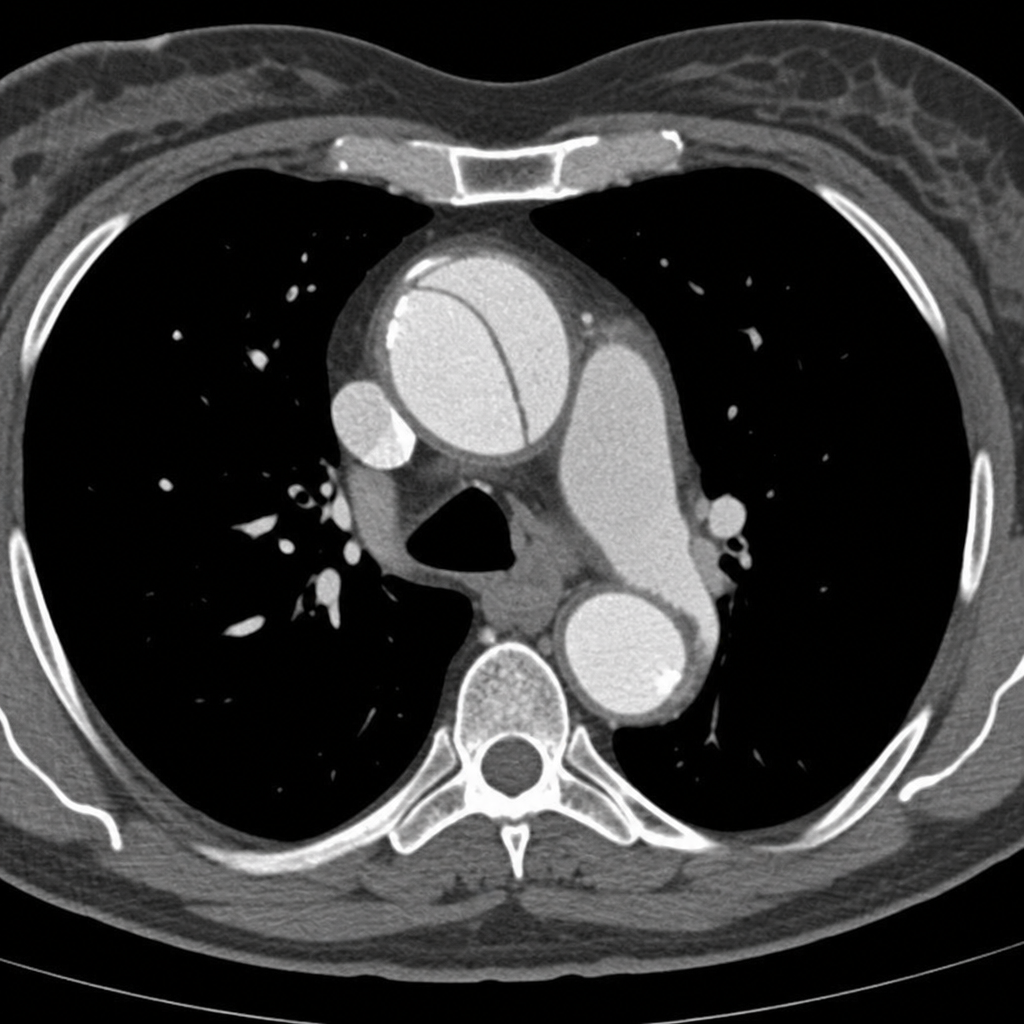
A 45-year-old woman presents to the emergency department with sudden-onset severe tearing chest pain radiating to the interscapular region. Her blood pressure is 178/96 mmHg in the right arm and 142/80 mmHg in the left arm. She is diaphoretic and in moderate distress. A CT angiogram of the chest is obtained and demonstrates an intimal flap involving the ascending aorta, consistent with a Stanford Type A aortic dissection. Based on the imaging findings, which of the following is the most appropriate next step in management?
Practice by Chapter
Donor selection criteria
Practice Questions
Brain death criteria
Practice Questions
Organ preservation techniques
Practice Questions
Immunosuppression principles
Practice Questions
Rejection diagnosis and management
Practice Questions
Liver transplantation
Practice Questions
Kidney transplantation
Practice Questions
Heart transplantation
Practice Questions
Lung transplantation
Practice Questions
Pancreas and islet cell transplantation
Practice Questions
Small bowel transplantation
Practice Questions
Post-transplant infections
Practice Questions
Long-term complications of transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app