
Pulmonary complications — MCQs

Five days after being admitted to the hospital for an open cholecystectomy, a 56-year-old woman develops difficulty breathing. She also has fevers, chills, and malaise. She has a cough productive of minimal amounts of yellowish-white sputum that started two days prior. She has type 2 diabetes mellitus, hypertension, and a history of gallstones. Her current medications include metformin, lisinopril, and atorvastatin. Her temperature is 39.5°C (103.1°F), pulse is 104/minute, blood pressure is 94/68 mm Hg, and respirations are 30/minute. Pulse oximetry on 2 L of oxygen via nasal cannula shows an oxygen saturation of 92%. Examination reveals decreased breath sounds over the right lung base. Abdominal examination shows a well-healing scar without erythema or discharge in the right upper quadrant. The skin is warm and well-perfused. Her hemoglobin concentration is 10.5 g/dL, leukocyte count is 16,000/mm3, platelet count is 345,000/mm3, and creatinine is 1.5 mg/dL. She is admitted to the ICU and started on IV fluids. Blood and urine for cultures are obtained. X-ray of the chest reveals a right sided pleural effusion. Which of the following is the next best step in management?
A previously healthy 35-year-old woman is brought into the emergency department after being found unresponsive by her husband. Her husband finds an empty bottle of diazepam tablets in her pocket. She is stuporous. At the hospital, her blood pressure is 90/40 mm Hg, the pulse is 58/min, and the respirations are 6/min. The examination of the pupils shows normal size and reactivity to light. Deep tendon reflexes are 1+ bilaterally. Babinski sign is absent. All 4 extremities are hypotonic. The patient is intubated and taken to the critical care unit for mechanical ventilation and treatment. Regarding the prevention of pneumonia in this patient, which of the following strategies is most likely to achieve this goal?
Three days after undergoing coronary artery bypass surgery, a 72-year-old man has severe right upper quadrant pain, fever, nausea, and vomiting. He has type 2 diabetes mellitus, benign prostatic hyperplasia, peripheral vascular disease, and chronic mesenteric ischemia. He had smoked one pack of cigarettes daily for 30 years but quit 10 years ago. He drinks 8 cans of beer a week. His preoperative medications include metformin, aspirin, simvastatin, and finasteride. His temperature is 38.9°C (102°F), pulse is 102/min, respirations are 18/min, and blood pressure is 110/60 mmHg. Auscultation of the lungs shows bilateral inspiratory crackles. Cardiac examination shows no murmurs, rubs or gallops. Abdominal examination shows soft abdomen with tenderness and sudden inspiratory arrest upon palpation in the right upper quadrant. There is no rebound tenderness or guarding. Laboratory studies show the following: Hemoglobin 13.1 g/dL Hematocrit 42% Leukocyte count 15,700/mm3 Segmented neutrophils 65% Bands 10% Lymphocytes 20% Monocytes 3% Eosinophils 1% Basophils 0.5% AST 40 U/L ALT 100 U/L Alkaline phosphatase 85 U/L Total bilirubin 1.5 mg/dL Direct 0.9 mg/dL Amylase 90 U/L Abdominal ultrasonography shows a distended gallbladder, thickened gallbladder wall with pericholecystic fluid, and no stones. Which of the following is the most appropriate next step in management?
A 52-year-old man presents to the emergency department with sudden-onset dyspnea, tachypnea, and chest pain. He works as a long-haul truck driver, and he informs you that he recently returned to the west coast from a trip to Tennessee. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type 2, and mild intellectual disability. He currently smokes 2 packs of cigarettes/day, drinks a 6-pack of beer/day, and he endorses a past history of injection drug use but currently denies any illicit drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 23/min. His physical examination shows minimal bibasilar rales, but otherwise clear lungs on auscultation, grade 2/6 holosystolic murmur, and a benign abdominal physical examination. A computed tomography angiography (CTA) demonstrates a segmental pulmonary embolism (PE). Which of the following is the most appropriate treatment plan for this patient?
A 43-year-old woman presents to her primary care physician with complaints of mild shortness of breath and right-sided chest pain for three days. She reports that lately she has had a nagging nonproductive cough and low-grade fevers. On examination, her vital signs are: temperature 99.1 deg F (37.3 deg C), blood pressure is 115/70 mmHg, pulse is 91/min, respirations are 17/min, and oxygen saturation 97% on room air. She is well-appearing, with normal work of breathing, and no leg swelling. She is otherwise healthy, with no prior medical or surgical history, currently taking no medications. The attending has a low suspicion for the most concerning diagnosis and would like to exclude it with a very sensitive though non-specific test. Which of the following should this physician order?
A 68-year-old woman presents to the hospital for an elective right hemicolectomy. She is independently mobile and does her own shopping. She has had type 2 diabetes mellitus for 20 years, essential hypertension for 15 years, and angina on exertion for 6 years. She has a 30-pack-year history of smoking. The operation was uncomplicated. On post-op day 5, she becomes confused. She has a temperature of 38.5°C (101.3°F), respiratory rate of 28/min, and oxygen saturation of 92% on 2 L of oxygen. She is tachycardic at 118/min and her blood pressure is 110/65 mm Hg. On chest auscultation, she has coarse crackles in the right lung base. Her surgical wound appears to be healing well, and her abdomen is soft and nontender. Which of the following is the most likely diagnosis?
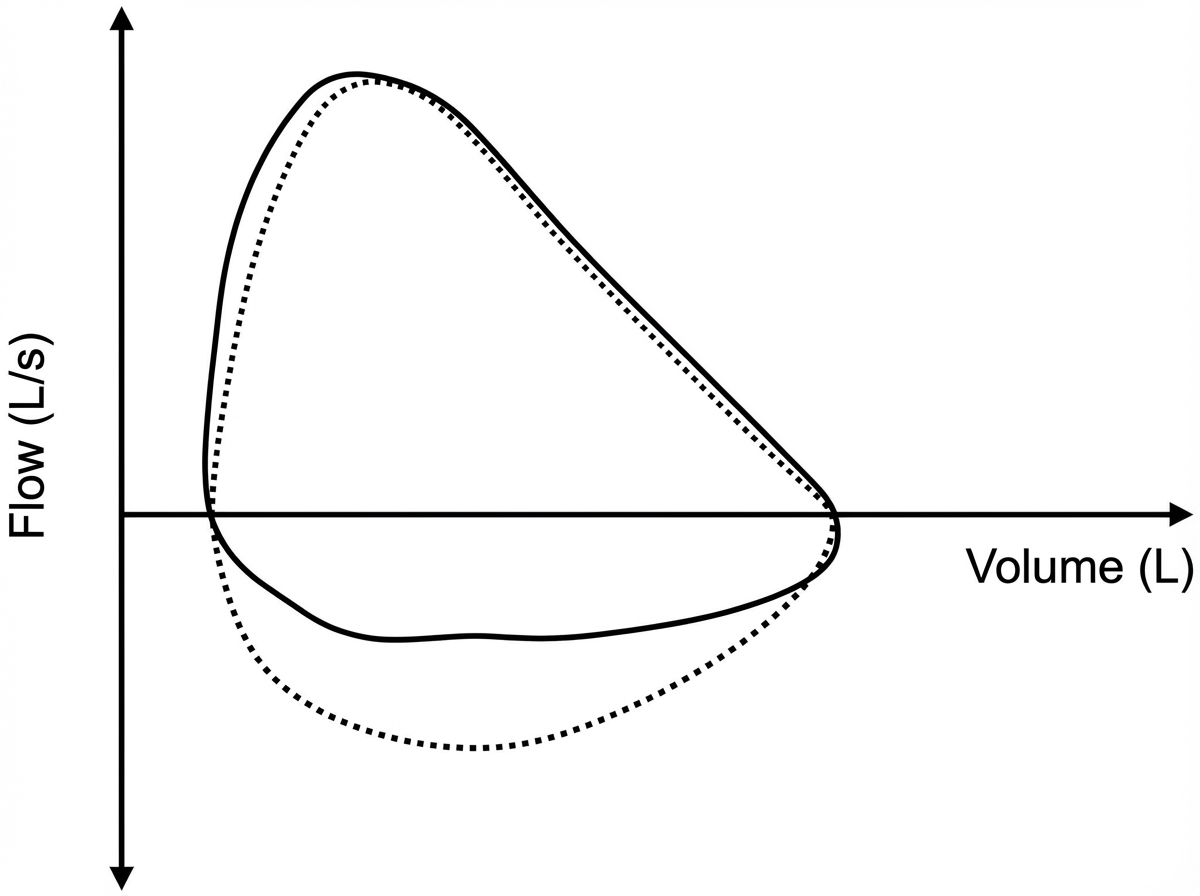
Five minutes after arriving in the postoperative care unit following total knee replacement under general anesthesia, a 55-year-old woman is acutely short of breath. The procedure was uncomplicated. Postoperatively, prophylactic treatment with cefazolin was begun and the patient received morphine and ketorolac for pain management. She has generalized anxiety disorder. Her only other medication is escitalopram. She has smoked one pack of cigarettes daily for 25 years. Her temperature is 37°C (98.6°F), pulse is 108/min, respirations are 26/min, and blood pressure is 95/52 mm Hg. A flow-volume loop obtained via pulmonary function testing is shown. Which of the following is the most likely underlying cause of this patient's symptoms?
A 55-year-old man presents to his primary care physician for a wellness checkup. The patient has a past medical history of alcohol abuse and is currently attending alcoholics anonymous with little success. He is currently drinking roughly 1L of hard alcohol every day and does not take his disulfiram anymore. Which of the following findings is most likely to also be found in this patient?
A 5-year-old child is brought to a pediatric clinic by his mother for a rash that started a few days ago. The mother adds that her son has also had a fever and sore throat since last week. His immunizations are up to date. On examination, a rash is present over the trunk and upper extremities and feels like sandpaper to touch. An oropharyngeal examination is suggestive of exudative pharyngitis with a white coat over the tongue. The physician swabs the throat and uses the swab in a rapid antigen detection test kit. He also sends the sample for microbiological culture. The physician then recommends empiric antibiotic therapy and tells the mother that if the boy is left untreated, the likelihood of developing a complication later in life is very high. Which of the following best explains the mechanism underlying the development of the complication the physician is talking about?
A 31-year-old woman is brought to the emergency department 25 minutes after sustaining a gunshot wound to the neck. She did not lose consciousness. On arrival, she has severe neck pain. She appears anxious. Her temperature is 37°C (98.6°F), pulse is 105/min, respirations are 25/min, and blood pressure is 100/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. She is oriented to person, place, and time. Examination shows a bullet entrance wound in the right posterior cervical region of the neck. There is no exit wound. Carotid pulses are palpable bilaterally. There are no carotid bruits. Sensation to pinprick and light touch is normal. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. In addition to intravenous fluid resuscitation, which of the following is the most appropriate next step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app