
Ileus and bowel dysfunction — MCQs

A 75-year-old male is hospitalized for bloody diarrhea and abdominal pain after meals. Endoscopic work-up and CT scan lead the attending physician to diagnose ischemic colitis at the splenic flexure. Which of the following would most likely predispose this patient to ischemic colitis:
A 38-year-old man arrives at the emergency department with severe periumbilical, colicky pain and abdominal distention for the past 2 days. He is nauseated and reports vomiting light-green emesis 8 times since yesterday morning. He has not had a bowel movement or passed any gas for the past 3 days. He has a past medical history of ventral hernia repair 5 years ago. His heart rate is 110/min, respiratory rate is 24/min, temperature is 38.0°C (100.4°F), and blood pressure is 120/90 mm Hg. The abdomen is distended and mildly tender to deep palpation. Bowel sounds are high-pitched and tinkling. Which of the following is the most likely cause?
A 32-year-old man comes to the emergency department because of recurrent episodes of vomiting for 1 day. He has had over 15 episodes of bilious vomiting. During this period he has had cramping abdominal pain but has not had a bowel movement or passed flatus. He does not have fever or diarrhea. He was diagnosed with Crohn disease at the age of 28 years which has been well controlled with oral mesalamine. He underwent a partial small bowel resection for midgut volvulus at birth. His other medications include vitamin B12, folic acid, loperamide, ferrous sulfate, and vitamin D3. He appears uncomfortable and his lips are parched. His temperature is 37.1°C (99.3°F), pulse is 103/min, and blood pressure is 104/70 mm Hg. The abdomen is distended, tympanitic, and tender to palpation over the periumbilical area and the right lower quadrant. Rectal examination is unremarkable. A CT scan of the abdomen shows multiple dilated loops of small bowel with a transition zone in the mid to distal ileum. After 24 hours of conservative management with IV fluid resuscitation, nasogastric bowel decompression, promethazine, and analgesia, his condition does not improve and a laparotomy is scheduled. During the laparotomy, two discrete strictures are noted in the mid-ileum, around 20 cm apart. Which of the following is the most appropriate next step in management?
Four days after undergoing a total abdominal hysterectomy for atypical endometrial hyperplasia, a 59 year-old woman reports abdominal bloating and discomfort. She has also had nausea without vomiting. She has no appetite despite not having eaten since the surgery and drinking only sips of water. Her postoperative pain has been well controlled on a hydromorphone patient-controlled analgesia (PCA) pump. Her foley was removed on the second postoperative day and she is now voiding freely. Although she lays supine in bed for most of the day, she is able to walk around the hospital room with a physical therapist. Her temperature is 36.5°C (97.7°F), pulse is 84/min, respirations are 10/min, and blood pressure is 132/92 mm Hg. She is 175 cm (5 ft 9 in) tall and weighs 115 kg (253 lb); BMI is 37.55 kg/m2. Examination shows a mildly distended, tympanic abdomen; bowel sounds are absent. Laboratory studies are within normal limits. An x-ray of the abdomen shows uniform distribution of gas in the small bowel, colon, and rectum without air-fluid levels. Which of the following is the most appropriate next step in the management of this patient?
A 59-year-old healthy woman presents to her primary care physician’s office six weeks after undergoing an elective breast augmentation procedure in the Dominican Republic. She was told by her surgeon to establish post-operative care once back in the United States. Today she is bothered by nausea and early satiety. Her past medical history is significant only for GERD for which she takes ranitidine. Since the surgery, she has also taken an unknown opioid pain medication that was given to her by the surgeon. She reports that she has been taking approximately ten pills a day. On examination she is afebrile with normal vital signs and her surgical incisions are healing well. Her abdomen is distended and tympanitic. The patient refuses to stop her pain medicine and laxatives are not effective; what medication could be prescribed to ameliorate her gastrointestinal symptoms?
A 56-year-old woman is one week status post abdominal hysterectomy when she develops a fever of 101.4°F (38.6°C). Her past medical history is significant for type II diabetes mellitus and a prior history of alcohol abuse. The operative report and intraoperative cystoscopy indicate that the surgery was uncomplicated. The nurse reports that since the surgery, the patient has also complained of worsening lower abdominal pain. She has given the patient the appropriate pain medications with little improvement. The patient has tolerated an oral diet well and denies nausea, vomiting, or abdominal distension. Her blood pressure is 110/62 mmHg, pulse is 122/min, and respirations are 14/min. Since being given 1000 mL of intravenous fluids yesterday, the patient has excreted 800 mL of urine. On physical exam, she is uncomfortable, shivering, and sweating. The surgical site is intact, but the surrounding skin appears red. No drainage is appreciated. The abdominal examination reveals tenderness to palpation and hypoactive bowel sounds. Labs and a clean catch urine specimen are obtained as shown below: Leukocyte count and differential: Leukocyte count: 18,000/mm^3 Segmented neutrophils: 80% Bands: 10% Eosinophils: 1% Basophils: < 1% Lymphocytes: 5% Monocytes: 4% Platelet count: 300,000/mm^3 Hemoglobin: 12.5 g/dL Hematocrit: 42% Urine: Epithelial cells: 15/hpf Glucose: positive RBC: 1/hpf WBC: 2/hpf Bacteria: 50 cfu/mL Ketones: none Nitrites: negative Leukocyte esterase: negative Which of the following is most likely the cause of this patient’s symptoms?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 36-year-old man is seen in the emergency department for back pain that has been getting progressively worse over the last 4 days. Upon further questioning, he also notes that he has been having a tingling and burning sensation rising up from his feet to his knees bilaterally. The patient states he is having difficulty urinating and having bowel movements over the last several days. His temperature is 97.4°F (36.3°C), blood pressure is 122/80 mmHg, pulse is 85/min, respirations are 14/min, and oxygen saturation is 98% on room air. Physical exam is notable for weak leg flexion bilaterally along with decreased anal sphincter tone. Which of the following is the best next step in management?
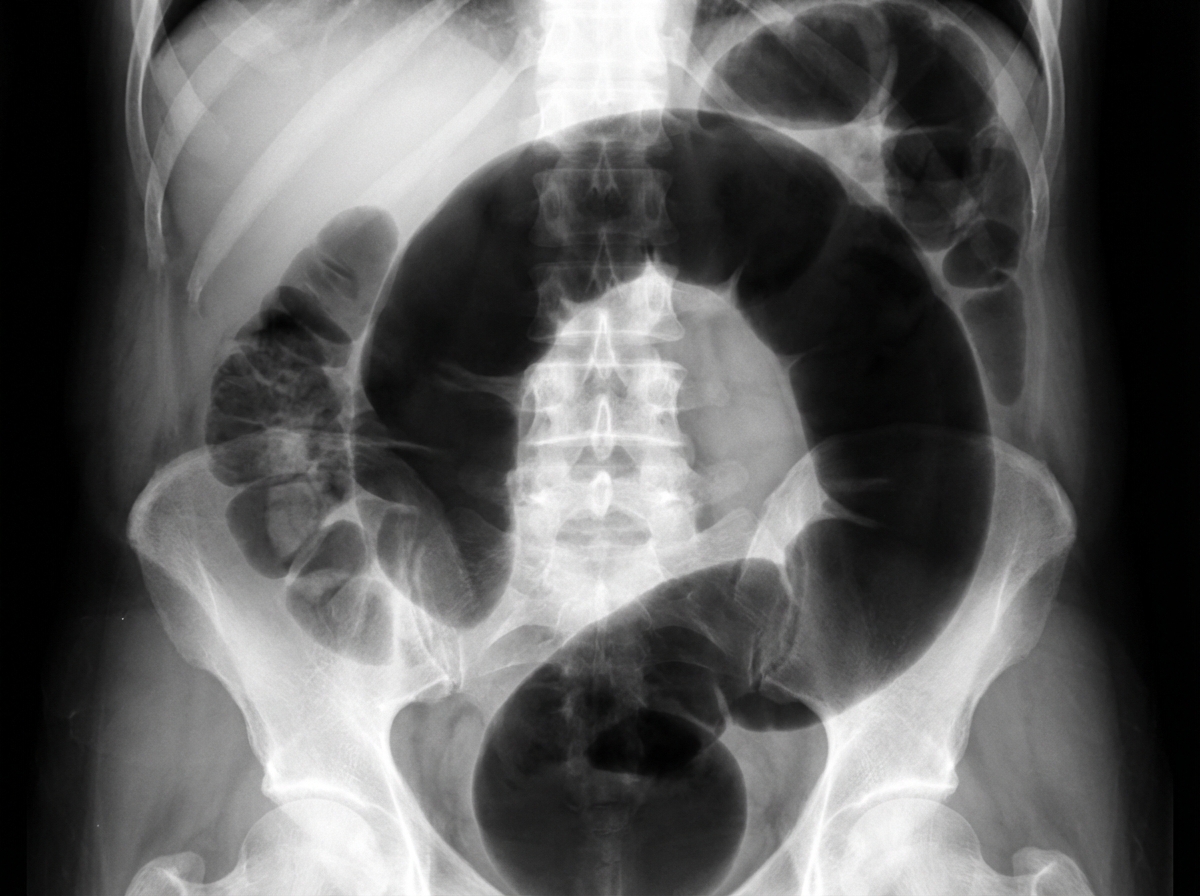
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
A 32-year-old Caucasian female is admitted to the emergency department with a 48-hour history of severe and diffuse abdominal pain, nausea, vomiting, and constipation. Her personal history is unremarkable except for an ectopic pregnancy 5 years ago. Upon admission, she is found to have a blood pressure of 120/60 mm Hg, a pulse of 105/min, a respiratory rate 20/min, and a body temperature of 37°C (98.6°F). She has diffuse abdominal tenderness, hypoactive bowel sounds, and mild distention on examination of her abdomen. Rectal and pelvic examination findings are normal. What is the most likely cause of this patient's condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app